Clinician Perspectives on Type 1 Diabetes Guidelines and Glucose Data Interpretation
This study explored healthcare professionals' perspectives on the management of Type 1 Diabetes Mellitus (T1DM) through a two-part questionnaire. The first part examined how clinicians prioritise and apply current clinical guidelines, including the r…
Authors: Mohammed Basheikh, Rujiravee Kongdee, Hood Thabit
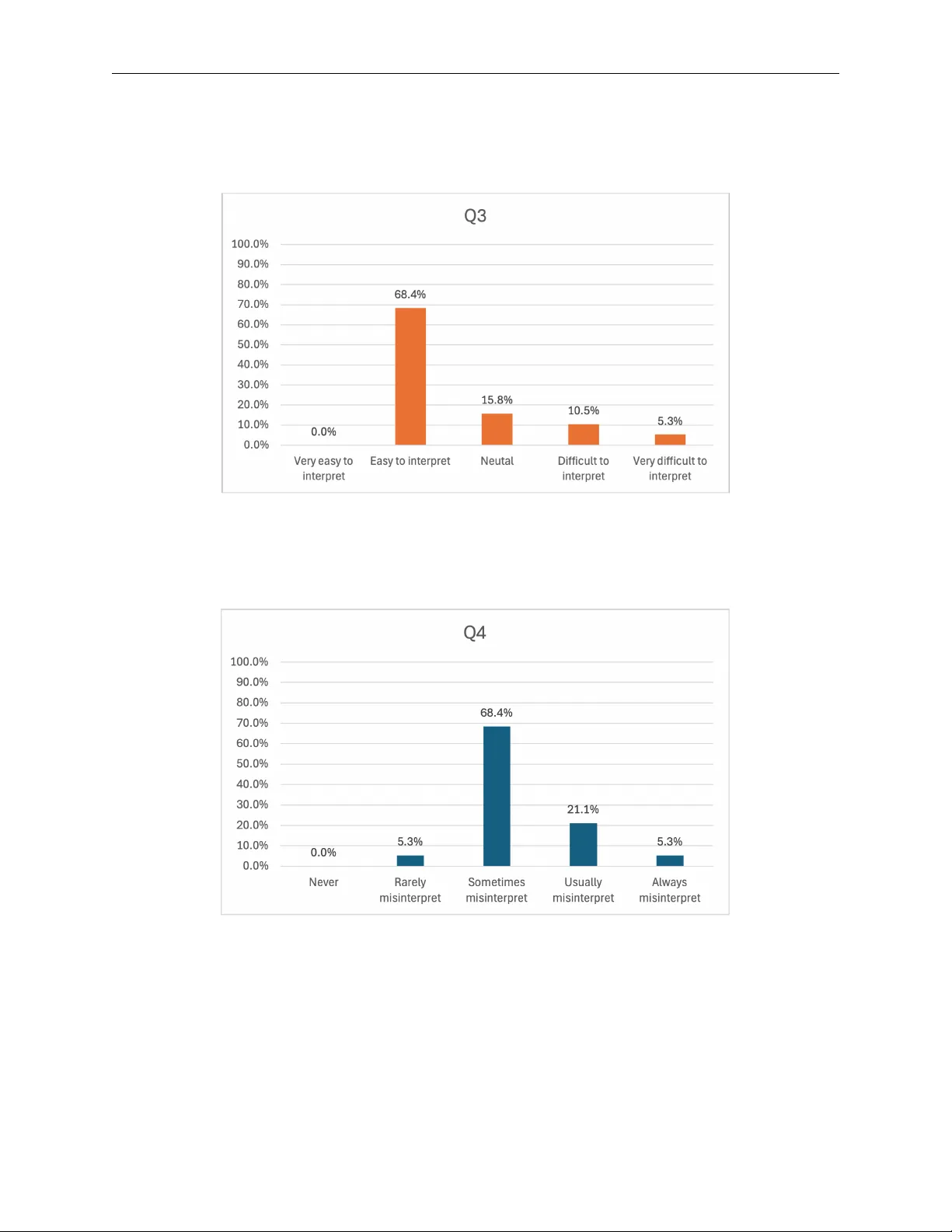
C L I N I C I A N P E R S P E C T I V E S O N T Y P E 1 D I A B E T E S G U I D E L I N E S A N D G L U C O S E D A T A I N T E R P R E T A T I O N Mohammed Basheikh 1 ∗ , Rujirav ee Kongdee 1 † , Hood Thabit 2,3 , Bijan Parsia 1 , Sarah Clinch 1 , Simon Harper 1 1 Department of Computer Science, University of Manchester , UK 2 Diabetes, Endocrine and Metabolism Centre, Manchester Uni versity NHS F oundation T rust 3 Division of Diabetes, Endocrinology and Gastr oenterology , University of Manchester , UK March 27, 2026 A B S T R AC T This study explored healthcare professionals’ perspecti ves on the management of T ype 1 Diabetes Mellitus (T1DM) through a two-part questionnaire. The first part examined ho w clinicians prioritise and apply current clinical guidelines, including the relati ve importance assigned to dif ferent aspects of T1DM management. The second part in vestigated clinicians’ perceptions of patients’ ability to interpret data from the glucose monitoring devices and to make appropriate treatment decisions. An online questionnaire was completed by 19 healthcare professionals working in diabetes-related roles in the United Kingdom. The findings re vealed that blood glucose management is prioritised within clinical guidance and that advice is frequently tailored to individual patient needs. Additionally , clinicians generally percei ve that data presented in glucose monitoring de vices is easy for patients to interpret and based on these data, the y belie ve that patients occasionally mak e correct treatment decisions. Keyw ords T ype 1 Diabetes · Medical guidelines · Healthcare professionals · Self-management · Glucose monitoring devices · Interpretation · Questionnaire 1 Introduction T ype 1 Diabetes Mellitus (T1DM) is a chronic autoimmune disease that attacks the pancreas’ s beta-cells, inhibiting insulin production and preventing the body from self-re gulating blood glucose le vels [ 1 ]. The Juvenile Diabetes Research Foundation (JDRF) suggest that roughly 400,000 people liv e with T1DM in the UK [ 6 ]. It is estimated the National Health Service (NHS) has spent around £1.92 billion in the last decade for diabetes treatment [ 2 ]. It is considered that due to the chronic complications resulting from poor glycaemic control, the risk of mortality of a person with type 1 diabetes is higher when compared to a non-diabetic counterpart [ 10 ]. For those li ving with T1DM to achiev e the stringent glycaemic control needed to mitigate this increased mortality risk, blood glucose le vels need to be monitored regularly and adjusted with either e xogenous insulin or consuming a glucose source. Less than 60% of people with T1DM achiev e the desired glycaemic target ranges to mitig ate the risk of T1DM complications [14]. The National Institute for Health and Care Excellence (NICE) guideline offers comprehensiv e care and treatment recommendations for adults with type 1 diabetes [ 10 ], which many healthcare professionals adopt to clinically manage those with type 1 diabetes. Despite the guideline’ s comprehensi veness, there are v arious aspects of diabetes management that healthcare professionals must consider , such as dietary management, physical activity , blood glucose management and mitigating cardiov ascular risk. In addition to guidelines, glucose self-monitoring is crucial for maintaining safe glycaemic lev els. Diabetes technologies, which include wearable glucose monitoring devices, ha ve been de veloped to assist people living with T1DM to reduce glycaemic variation while impro ving quality of life [ 11 ]. Currently , there are three major types of blood glucose ∗ CONT A CT Mohammed Basheikh. Email: mohammed.basheikh@postgrad.manchester .ac.uk † CONT A CT Rujiravee K ongdee. Email: rujiravee.k ongdee@manchester .ac.uk Clinician Perspectiv es on T ype 1 Diabetes Guidelines and Glucose Data Interpretation monitoring systems: self-monitoring of blood glucose (SMBG), and continuous glucose monitoring (CGM) [ 3 , 5 ]. CGM devices ha ve become widely adopted due to the limitations of SMBG and the con venience of continuous glucose data they pro vide. SMBG users have to tak e a drop of blood and place it into a strip of a glucometer to see the reading many times a day , which causes pain and is time-consuming Despite the con venience of CGM devices, their applications’ user interface has been reported to be problematic. Research has shown that the interface demands excessi ve cognitiv e effort, is dif ficult to interpret, and requires substantial time to extract meaningful information ef fecti vely [ 8 , 7 , 12 ]. These are concerning because people living with T1DM hea vily rely on these user interfaces, and misinterpretation of data may result in delayed or inappropriate treatment, leading to life-threatening situations [4]. In this study , we sought to understand clinicians’ perspecti ves on implementing recommended guidelines and their perceptions of patients’ problems associated with current blood glucose monitoring devices among patients with type 1 diabetes. Accordingly , the focus of this work is two-fold. First, to identify the relati ve importance that healthcare professionals assign to the advice presented in the NICE guidelines. Second, to explore their opinions re garding problems in understanding the glucose monitoring devices in their patients. 2 Method 2.1 P articipant recruitment T o be eligible for the study , participants were required to be healthcare professionals working in a diabetes-related field and familiar with the NICE NG17 (T ype 1 diabetes in adults: diagnosis and management) guidelines. Participants were recruited through the Manchester Diabetes Centre. In addition, recruitment notices were posted on official medical websites, including those of the Association of British Clinical Diabetologists and Diabetes UK. 2.2 Data collection The study was conducted as an online questionnaire administered via the Qualtrics platform and required approximately 10 minutes to complete. The questionnaire consisted of 3 main parts: (1) Demographics, (2) T1DM guidelines and (3) Glucose monitoring devices. T able 1 presents the list of questions. Part Question Question type Demographic Please select your position Multiple choice (single answer): # Consultant Physician # Specialist Registrar # GP # Practice nurse # Specialist Nurse Practitioner (Diabetes) – Hos- pital/Community care # Specialist Nurse Practitioner (Diabetes) – Pri- mary/Community care # Dietitian # Other (please specify) Please specify your workplace or hospital post- code (first three letters; if not in the United King- dom, please specify your country) Free-text response Continued on next page 2 Clinician Perspectiv es on T ype 1 Diabetes Guidelines and Glucose Data Interpretation Part Question Question type T1DM guidelines Q1. Do you change your self-management advice for people with type 1 diabetes based on each individual’ s needs and condition? Multiple choice (multiple answers): □ I follo w the national standards and guidance. □ I follo w local practice guidance. □ I always follo w the national standards and guidance and rarely change my advice accord- ing to patient’ s clinical or personal needs. □ I always follow local practice guidance and rarely change my advice according to patient’ s clinical or personal needs. □ I always adjust my advice according to pa- tient’ s clinical or personal needs. Please describe further (Free-text response) Q2. Based on current T ype 1 Diabetes guidance (e.g., NICE NG17, American Diabetes Associa- tion, European Association for the Study of Dia- betes), which information do you consider most helpful to support clinical management in adults ov er 25 years with T ype 1 Diabetes? (Rank from 1 = most important to 5 = least important) Rank order: • Dietary management • Physical acti vity • Blood glucose management • Insulin therapy and deli very • Hypoglycaemia aw areness and management Glucose monitor- ing devices Q3. T o what extent do you think blood glucose data presented in continuous and flash glucose monitoring systems are difficult to interpret for patients with type 1 diabetes? 5-point Likert scale: • V ery difficult to interpret • Dif ficult to interpret • Neither dif ficult nor easy to interpret • Easy to interpret • V ery easy to interpret Q4. How often do you think patients with type 1 diabetes misinterpret their blood glucose data from monitoring systems? 5-point Likert scale: • Ne ver • Rarely • Sometimes • Usually • Always Q5. T o what extent do you think patients with type 1 diabetes correctly decide on the action to take in response to their blood glucose le vels? 5-point Likert scale: almost always correct; usually cor- rect; occasionally correct; usually not correct; almost nev er correct • Almost always correct • Usually correct • Occasionally correct • Usually not correct • Almost nev er correct T able 1: List of questions and response formats 2.3 Ethical appr oval This study was re viewed and approv ed by the Uni versity of Manchester Research Ethics Committee before data collection be gan (Reference number: 2023-15646-27225). All participants provided informed consent for their data to be published. 3 Clinician Perspectiv es on T ype 1 Diabetes Guidelines and Glucose Data Interpretation 3 Findings 3.1 P articipants demographics A total of 19 healthcare professionals completed the questionnaire. The number of respondents in each role is outlined in T able 2. Role Respondents Consultant Physician 7 Specialist Registrar 4 GP 2 Specialist Nurse Practitioner (Diabetes) – Hospital/Community care 1 Specialist Nurse Practitioner (Diabetes) – Primary/Community care 2 Dietitian 2 Other (Retired GP who worked as medical advisor) 1 T able 2: Number of respondents in each role In terms of the specified workplace, participants were geographically distributed across sev eral regions in England, with a concentra- tion in the North W est (see the Appendix). 3.2 T1DM Guidelines Q1: Do you change your self-management advice for people with type 1 diabetes based on each indi vidual’ s needs and condition? The results are as follows: • I always adjust my advice according to patient’ s clinical or personal needs: 36.36% • I always follow local practice guidance and rarely change my advice according to patient’ s clinical or personal needs: 6.06% • I always follo w the national standards and guidance and rarely change my advice according to patient’ s clinical or personal needs: 9.09% • I follo w local practice guidance: 18.18% • I follo w the national standards and guidance: 30.30% Q2: Based on current T ype 1 Diabetes guidance (eg: National Institute for Health and Care Excellence - NG17, American Diabetes Association or European Association for the Study of Diabetes) which information from these guidance do you consider most helpful to support your clinical management in adults (ov er age of 25) with T ype 1 Diabetes. (Rank the list, ’1’ is the most important and ’5’ is the least important) The results are presented in T able 3 : Rank Clinical Management Area 1 2 3 4 5 Dietary management 0 4 4 10 1 Physical acti vity 1 2 2 1 13 Blood glucose management 9 3 3 3 1 Insulin therapy and deli very 7 8 0 2 2 Hypoglycaemia awareness and management 2 2 10 3 2 T able 3: Clinician prioritisation of T ype 1 diabetes management guidelines The results suggest that most clinicians report adapting their self-management recommendations for people with T1DM according to individual clinical and personal circumstances. The questions specifically referred to clinician-led decisions that doctors ha ve the authority to modify . Only a small proportion indicated that the y rarely adjust their advice and instead primarily adhere to local or national guidance. These findings suggest that personalised clinical judgement is prioritised in routine practice when clinicians have discretion to individualise care. Also, the results show agreement among healthcare professionals regarding the prioritisation of current T1DM guidance. Blood glucose management was considered the most important aspect, while dietary management and physical activity were considered the least important. These findings indicate that dietary management and physical activity are giv en lower priority in clinical practice. 4 Clinician Perspectiv es on T ype 1 Diabetes Guidelines and Glucose Data Interpretation 3.3 Glucose Monitoring De vices Q3: T o what extent do you think blood glucose data presented in continuous and flash glucose monitoring systems are dif ficult to interpret for patients with type 1 diabetes? The results are depicted in Figure 1. Figure 1: Distribution of respondents’ perceptions of the difficulty of interpreting data presented in continuous and flash glucose monitoring devices (Q3). Q4: Ho w often do you think patients with type 1 diabetes misinterpret their blood glucose data from monitoring systems? The results are shown in Figure 2. Figure 2: Distribution of respondents’ perceptions of the frequenc y that patients misinterpret their data presented in monitoring devices (Q4). Q5: T o what e xtent do you think patients with type 1 diabetes correctly decide on the action to tak e in response to their blood glucose lev els? The results are presented in Figure 3. The results suggest that the majority of respondents believ e that interpreting data presented by CGM and/or Flash is easy for patients. Howe ver , they also consider that patients sometimes misinterpret the data. With respect to treatment decision-making, most respondents think that patients only occasionally make correct decisions. The belief that data presented by CGM and/or Flash systems should be easy for people with T1DM to interpret contrasts with findings from empirical research. In one study , semi-structured interviews were conducted with participants with T1DM, who were asked to provide spontaneous v erbal interpretations of CGM and Flash user interfaces. The results showed that participants correctly 5 Clinician Perspectiv es on T ype 1 Diabetes Guidelines and Glucose Data Interpretation Figure 3: Distribution of respondents’ perceptions of the frequency that patients correctly mak e treatment decisions based on their glucose lev els (Q5). interpreted the displayed glucose data in fewer than 40% of cases. Furthermore, the correctness of treatment decisions was e ven lower , at 22% [ 9 ]. These findings suggest that, although healthcare professionals may perceiv e such data as straightforward to interpret, people with T1DM often experience substantial difficulty . Consistent with this, prior research has also reported that while these individuals face challenges in interpreting these de vices, healthcare providers tend to assume that this task is straightforward [13]. This highlights a clear misalignment between patient and clinician perspectives. There is a need for healthcare professionals to reassess their assumptions, as patients may not interpret glucose data as effecti vely as clinicians expect. Moreover , other factors such as patients’ age, nativ e language and socioeconomic background could also affect the interpretability of their device data. These insights can be used to support more targeted and ef fectiv e clinical con versations to help patients understand their data more accurately . 4 Data A vailability The dataset is av ailable in a Zenodo Repository ‘Clinicans-perspecti ve-T1DM’ at https://doi.org/10.5281/zenodo.18404347 5 Acknowledgement The authors would like to thank all participants for their time and contribution to this study . Mohammed Basheikh was supported by the Univ ersity of Jeddah, Saudi Arabia. Rujirav ee K ongdee was supported by the Royal Thai Go vernment Scholarship. References [1] A T K I N S O N , M . A . , E I S E N B A RT H , G . S . , A N D M I C H E L S , A . W . T ype 1 diabetes. The lancet 383 , 9911 (2014), 69–82. [2] A U T H O R I T Y , N . B . S . Prescribing for diabetes – england – 2015/16 to 2024/25. https://media.nhsbsa.nhs.uk/press- releases/e29454d6- 7346- 4183- b9fe- 57a31a04ce1e/ nhs- diabetes- treatment- spending- reaches- 1- 92- billion- as- new- medications- become- available , 8 2025. [Accessed 06-03-2026]. [3] C A P P O N , G . , V E T T O R E T T I , M . , S PA R A C I N O , G . , A N D F AC C H I N E T T I , A . Continuous glucose monitoring sensors for diabetes management: a re view of technologies and applications. Diabetes & metabolism journal 43 , 4 (2019), 383. [4] E R B A C H , M . , F R E C K M A N N , G . , H I N Z M A N N , R . , K U L Z E R , B . , Z I E G L E R , R . , H E I N E M A N N , L . , A N D S C H N E L L , O . Interferences and Limitations in Blood Glucose Self-T esting: An Overvie w of the Current Kno wledge. Journal of Diabetes Science and T ec hnology 10 , 5 (Sept. 2016), 1161–1168. [5] H Á S K OV Á , A . , R A D O V N I C K Á , L . , P E T RU Ž E L K OV Á , L . , P A R K I N , C . G . , G RU N B E R G E R , G . , H O R OV Á , E . , N A V R Á T I L OV Á , V . , K Á D ˇ E , O . , M ATO U L E K , M . , P R Á Z N ` Y , M . , E T A L . Real-time CGM is superior to flash glucose monitoring for glucose control in type 1 diabetes: the corrida randomized controlled trial. Diabetes Care 43 , 11 (2020), 2744–2750. 6 Clinician Perspectiv es on T ype 1 Diabetes Guidelines and Glucose Data Interpretation [6] J D R F . It’ s no joke – getting the facts straight on type 1 diabetes | Breakthrough T1D UK — breakthrought1d.or g.uk. https: //breakthrought1d.org.uk/resources/its- no- joke- getting- the- facts- straight- on- type- 1- diabetes/ , 2026. [Accessed 20-01-2026]. [7] K ATZ , D . , D A LTO N , N . , H O L L A N D , S . , O ’ K A N E , A . A . , A N D P R I C E , B . A . Questioning the Reflection Paradigm for Diabetes Mobile Apps. eHealth 360° (Dec. 2016), 315–326. [8] K ATZ , D . , P R I C E , B . A . , H O L L A N D , S . , A N D D A LTO N , N . Data, Data Everywhere, and Still T oo Hard to Link: Insights from User Interactions with Diabetes Apps. CHI (Apr . 2018), 503. [9] K O N G D E E , R . , P AR S I A , B . , T H A B I T , H . , A N D H A R P E R , S . Glucose interpretation meaning and action GIMA: Insights to blood glucose user interface interpretation in type 1 diabetes. Digital Health 11 (2025), 20552076251332580. [10] N AT I O N A L I N S T I T U T E F O R H E A LT H A N D C A R E E X C E L L E N C E . Diabetes (type 1 and type 2) in childr en and young people: diagnosis and management . National Institute for Health and Care Excellence, 8 2023. NICE Guidelines NG18. [11] O V I E D O , S . , V E H Í , J . , C A L M , R . , A N D A R M E N G O L , J . A revie w of personalized blood glucose prediction strategies for T1DM patients. International journal for numerical methods in biomedical engineering 33 , 6 (2017), e2833. [12] P I C K U P , J . C . , F O R D H O L L O W A Y , M . , A N D S A M S I , K . Real-T ime Continuous Glucose Monitoring in T ype 1 Diabetes: A Qualitativ e Framew ork Analysis of Patient Narrati ves. Diabetes Car e 38 , 4 (4 2015), 544–550. [13] R A J , S . , N E W M A N , M . W., L E E , J . M . , A N D A C K E R M A N , M . S . Understanding indi vidual and collaborativ e problem-solving with patient-generated data: challenges and opportunities. Pr oceedings of the ACM on Human-Computer Interaction 1 , CSCW (2017), 1–18. [14] S H E R R , J . L . , L A FF E L , L . M . , L I U , J . , W O L F , W. , B I S P H A M , J . , C H A P M A N , K . S . , F I N A N , D . , T I T I E V S K Y , L . , L I U , T., H A G A N , K . , G AG L I A , J . , C H A N DA R A NA , K . , B E R G E N S TA L , R . , A N D P E T T U S , J . Sev ere hypoglycemia and impaired awareness of hypoglycemia persist in people with type 1 diabetes despite use of diabetes technology: Results from a cross- sectional surve y . Diabetes Care 47 , 6 (01 2024), 941–947. A A ppendix The number of respondents in each location was as follo ws: • Manchester : 6 • London : 2 • Maidstone, K ent : 1 • Rishton, Lancashire : 1 • Liver pool : 1 • Peterbor ough : 1 • Sheffield : 1 • Redhill : 1 • W orthing : 1 • Stev enage : 1 • W elwyn Garden City : 1 • Birmingham : 1 • St Helens : 1 • Southend-on-Sea : 1 7
Original Paper
Loading high-quality paper...
Comments & Academic Discussion
Loading comments...
Leave a Comment