Non-Pharmaceutical Interventions Reshape Network Immunization Outcomes
Herd immunity is shaped not only by the infection capacity of a spreading epidemic or the contact structure of the hosting population, but also by how and under what circumstances individuals acquire immunity. Immunization strategies may interact with ongoing non-pharmaceutical interventions, which commonly aim to reduce social contact numbers. We demonstrate that these interactions can induce unexpectedly strong and counterintuitive effects on herd immunity. We explore these phenomena on spatially embedded contact networks and uncover a reversal in the relative effectiveness of disease- versus vaccine-induced immunization schemes, highlighting the average number of contacts as a critical determinant of emerging herd immunity. In sparse geometric networks with limited degree heterogeneity, uniform vaccination proves most effective; however, as average contact numbers increase, naturally acquired immunity ultimately becomes the better strategy. We show that this phenomenon may emerge not only in synthetic networks but also in real-world mixing networks, observed during non-pharmaceutical intervention periods across multiple states of the United States.
💡 Research Summary
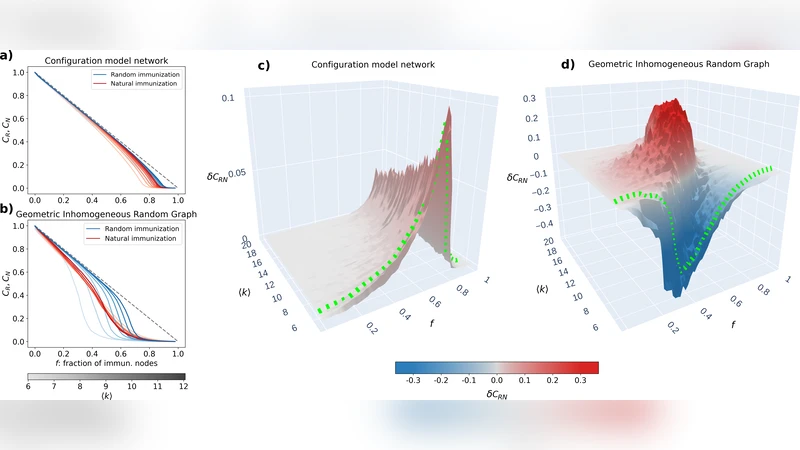
This paper investigates how non‑pharmaceutical interventions (NPIs) that reduce social contacts interact with the way individuals acquire immunity—through vaccination or natural infection—and how this interaction reshapes herd‑immunity outcomes on contact networks. The authors first construct spatially embedded geometric random graphs in which nodes are placed uniformly in a two‑dimensional plane and linked if they lie within a fixed radius. By varying node density and connection radius they generate networks with average degrees ranging from sparse (≈2) to dense (≈20), thereby spanning a continuum from highly homogeneous to moderately heterogeneous structures.
On each network they run stochastic SIR simulations and compare three immunization strategies: (1) Uniform Vaccination (UV), where a fixed proportion of the population is randomly immunized before the outbreak; (2) Natural Infection (NI), where immunity arises only after individuals recover from infection during the epidemic; and (3) Mixed, a combination of UV and NI with adjustable fractions. For each scenario they record the final immune coverage, the peak prevalence, and the total number of infections.
The central finding is a reversal in the relative effectiveness of UV versus NI as the average degree increases. In sparse networks (average degree ≤ 6) UV consistently outperforms NI: random vaccination cuts most transmission pathways, leading to a lower epidemic peak and higher final immunity. As the network becomes denser (average degree ≥ 8), multiple redundant paths emerge, making it harder for vaccination alone to block spread. In this regime NI becomes more efficient because natural infection simultaneously immunizes many nodes that lie on high‑degree hubs, rapidly dismantling the core of the transmission network. Consequently, the final immune coverage under NI surpasses that of UV, and the epidemic peak is reduced despite a larger number of initial infections. The Mixed strategy yields intermediate results, with its optimal composition depending on the precise average degree and the strength of NPIs.
To validate the synthetic‑network results, the authors analyze real‑world mobility and contact data from all 50 U.S. states during the 2020‑2021 COVID‑19 pandemic, a period marked by varying NPI policies (mask mandates, business closures, travel restrictions). They estimate state‑level average contact numbers from anonymized mobile‑phone movement and social‑media interaction proxies, then feed these estimates into the same SIR‑based framework. The empirical analysis reproduces the theoretical reversal: low‑density states such as Montana and Wyoming achieve higher herd immunity through vaccination campaigns, whereas high‑density states like New York and California see a larger contribution from natural infection after the initial wave, ultimately reaching comparable or higher immunity levels.
The paper draws several policy implications. First, the effectiveness of vaccination campaigns cannot be assessed in isolation; it must be calibrated against contemporaneous NPIs and the resulting average contact rate. Second, in high‑contact settings a controlled allowance of limited infection—sometimes termed “regulated natural immunity”—might accelerate herd‑immunity formation, but this approach carries substantial risks of severe disease and mortality, demanding careful ethical and health‑system capacity considerations. Third, real‑time monitoring of contact patterns (e.g., via mobility data) is essential for dynamically adjusting vaccine allocation, prioritizing high‑degree individuals when contacts are dense, and focusing on broad coverage when contacts are sparse.
Overall, the study highlights average degree as a pivotal determinant of herd‑immunity dynamics under combined pharmaceutical and non‑pharmaceutical interventions. By integrating network science with epidemiological modeling, it offers a nuanced framework for designing adaptive immunization strategies that reflect the evolving social contact landscape during pandemics.
Comments & Academic Discussion
Loading comments...
Leave a Comment