Temperature and Respiratory Emergency Department Visits: A Mediation Analysis with Ambient Ozone Exposure
High temperatures are associated with adverse respiratory health outcomes and increases in ambient air pollution. Limited research has quantified air pollution’s mediating role in the relationship between temperature and respiratory morbidity, such as emergency department (ED) visits. In this study, we conducted a causal mediation analysis to decompose the total effect of daily temperature on respiratory ED visits in Los Angeles from 2005 to 2016. We focused on ambient ozone as a mediator because its precursors and formation are directly driven by sunlight and temperature. We estimated natural direct, indirect, and total effects on the relative risk scale across deciles of temperature exposure compared to the median. We utilized Bayesian additive regression trees (BART) to flexibly characterize the nonlinear relationship between temperature and ozone and quantified uncertainty via posterior prediction and the Bayesian bootstrap. Our results showed that ozone partially mediated the association between high temperatures and respiratory ED visits, particularly at moderately high temperatures. We also validated our modeling approach through simulation studies. This study extends the existing literature by considering acute respiratory morbidity and employing a flexible modeling approach, offering new insights into the mechanisms underlying temperature-related health risks.
💡 Research Summary
This paper investigates how daily ambient temperature influences respiratory emergency department (ED) visits in Los Angeles County from 2005 to 2016, and quantifies the extent to which ambient ozone mediates that relationship. The authors adopt a causal mediation analysis framework, separating the total effect of temperature into a natural direct effect (NDE) that operates independently of ozone and a natural indirect effect (NIE) that operates through ozone formation. Ozone is chosen as the mediator because its photochemical production is directly driven by sunlight and temperature, making it a plausible mechanistic link between heat and respiratory morbidity.
The data set combines daily average temperature, daily 8‑hour maximum ozone concentrations, and counts of respiratory‑related ED visits obtained from public health, meteorological, and air‑quality monitoring agencies. Temperature exposure is categorized into deciles relative to the median, allowing the authors to explore non‑linear exposure‑response patterns across the full temperature distribution.
To model the potentially complex, non‑linear relationship between temperature and ozone, the authors employ Bayesian Additive Regression Trees (BART). BART is an ensemble of regression trees fitted within a Bayesian framework, which automatically captures interactions and non‑linearities without pre‑specifying functional forms. After fitting BART to the temperature‑ozone sub‑model, the authors propagate uncertainty using the Bayesian bootstrap to generate posterior predictive distributions for both the mediator and outcome models. These distributions are then used to compute posterior means and 95 % credible intervals for NDE, NIE, and the total effect (TE) on the relative risk (RR) scale.
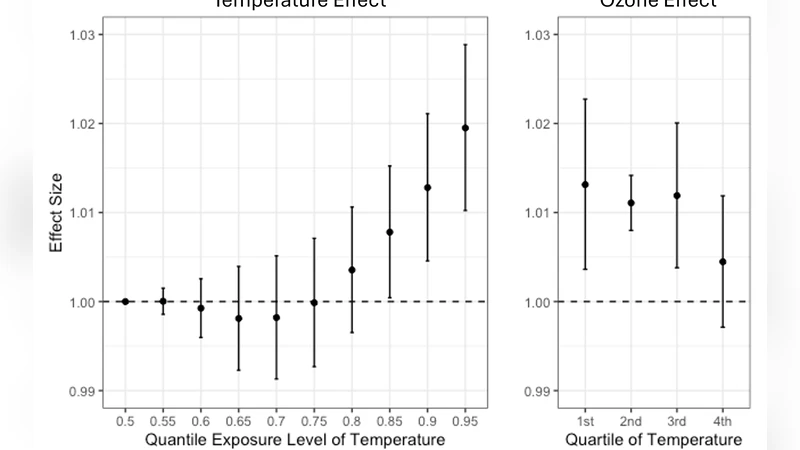
Results show a clear positive association between higher temperatures and increased respiratory ED visits. When temperature rises from the median to the 70th–80th percentile (approximately 28–30 °C), the indirect effect through ozone accounts for roughly 20–30 % of the total effect, indicating that ozone partially mediates the heat‑health relationship at moderate‑high temperatures. At the extreme high‑temperature tail (90th percentile and above, >33 °C), the direct effect dominates, suggesting that heat stress, dehydration, and other non‑pollution pathways become the primary drivers of respiratory visits. The mediation pattern is therefore temperature‑dependent: ozone plays a larger role at moderately high temperatures, while direct heat effects prevail at the hottest extremes.
To validate their approach, the authors conduct simulation studies in which the true direct and indirect effects are known. Applying the same BART‑mediated analysis to simulated data recovers the preset effects with minimal bias and appropriate coverage, confirming that the method can reliably disentangle non‑linear mediation in time‑series health data.
The paper acknowledges several limitations. First, only ozone is treated as a mediator; other pollutants such as PM₂.₅ or NO₂, which also respond to temperature, are omitted, potentially leading to omitted‑variable bias. Second, individual‑level exposure heterogeneity (e.g., time spent indoors, use of air‑conditioning) and socioeconomic confounders (e.g., access to care) are not directly controlled. Third, BART’s “black‑box” nature hampers straightforward interpretation of variable importance, and its computational demands may be prohibitive for larger spatial‑temporal datasets.
From a policy perspective, the findings suggest that strategies to mitigate heat‑related respiratory morbidity should address both the temperature itself and the ozone formation pathway. Measures could include stricter controls on ozone precursors (volatile organic compounds and NOₓ), urban greening to reduce surface temperatures, and targeted public health alerts on days when both temperature and ozone are forecasted to be high.
In summary, the study provides robust evidence that ambient ozone partially mediates the effect of high temperature on respiratory emergency visits, especially at moderate‑high temperature levels. By integrating causal mediation analysis with flexible Bayesian machine‑learning (BART), the authors advance methodological tools for environmental epidemiology and offer actionable insights for public‑health interventions in a warming climate.
Comments & Academic Discussion
Loading comments...
Leave a Comment