A Real-Time DDS-Based Chest X-Ray Decision Support System for Resource-Constrained Clinics
Internet of Things (IoT)-based healthcare systems offer significant potential for improving healthcare delivery in humanitarian and resource-constrained environments, providing essential services to underserved populations in remote areas. However, limited network infrastructure in such regions makes reliable communication challenging for traditional IoT systems. This paper presents a real-time chest X-ray decision support system designed for hospitals in remote locations. The proposed system integrates a fine-tuned ResNet50 deep learning model for disease classification with Fast DDS real-time middleware to ensure reliable and low-latency communication between healthcare practitioners and the inference system. Experimental results show that the model achieves an accuracy of 88.61%, precision of 88.76%, and recall of 88.49%. The system attains an average throughput of 3.2 KB/s and an average latency of 65 ms, demonstrating its suitability for deployment in bandwidth-constrained environments. These results highlight the effectiveness of DDS-based middleware in enabling real-time medical decision support for remote healthcare applications.
💡 Research Summary
The paper addresses the pressing need for reliable, real‑time medical decision support in humanitarian and resource‑constrained settings where network infrastructure is weak or intermittent. It proposes an end‑to‑end chest X‑ray (CXR) decision‑support system that couples a fine‑tuned ResNet‑50 convolutional neural network with Fast DDS, a high‑performance implementation of the Data Distribution Service (DDS) middleware.
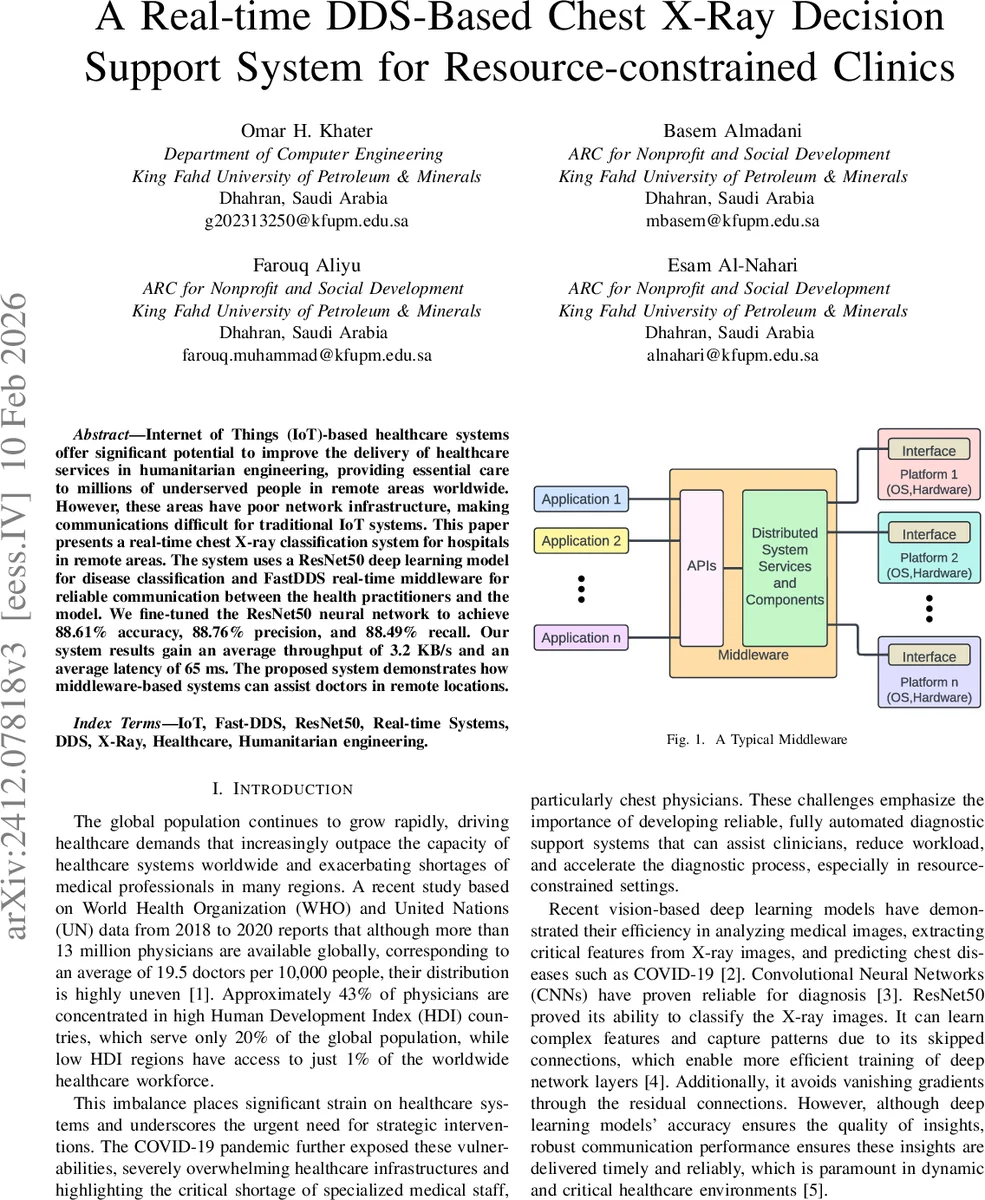
The system architecture consists of two logical nodes connected via a publish‑subscribe DDS bus. The “doctor node” runs on a Raspberry Pi, emulating a low‑power IoT device such as a smartphone; it publishes CXR images as DDS data samples and subscribes to diagnostic results. The “inference node” runs on a modest laptop, subscribes to the incoming images, performs inference with the ResNet‑50 model, and publishes the classification outcome back to the bus. All DDS entities are implemented in C++ and configured with QoS policies that guarantee reliable delivery and a tight latency budget.
Model development follows a transfer‑learning pipeline: a publicly available chest‑X‑ray dataset (e.g., NIH ChestX‑ray14) is used to pre‑train ResNet‑50, after which the final fully‑connected layer is replaced and the network is fine‑tuned on a curated multi‑class disease set. Data augmentation, learning‑rate scheduling, and early stopping are employed to mitigate over‑fitting. The resulting classifier achieves 88.61 % overall accuracy, 88.76 % precision, and 88.49 % recall—performance that, while lower than state‑of‑the‑art large‑scale models, is sufficient for triage‑level assistance in low‑resource clinics.
Network performance is evaluated under bandwidth‑constrained conditions that mimic 2G/3G mobile links. The Fast DDS middleware delivers an average end‑to‑end latency of 65 ms and a throughput of 3.2 KB s⁻¹, demonstrating that diagnostic feedback can be provided almost instantaneously even when the communication channel is narrow and potentially lossy.
A thorough literature review compares alternative middleware solutions. Lightweight frameworks such as Snout offer minimal CPU and memory footprints but lack scalability across geographically distributed nodes. High‑performance DDS variants combined with DPDK or XDP can reduce latency further, yet they introduce considerable setup complexity and maintenance overhead—undesirable traits for deployments in remote health centers. Hybrid JMS‑DDS architectures enable separation of real‑time and non‑real‑time traffic but depend on the Java ecosystem, reducing portability. The authors argue that Fast DDS strikes the best balance among real‑time guarantees, scalability, cross‑platform support, and operational simplicity for the target application.
Limitations acknowledged include the modest classification accuracy relative to newer architectures (e.g., EfficientNet, Vision Transformers) and the reliance of DDS on the operating‑system network stack, which may impede strict hard‑real‑time guarantees under extreme packet loss. Future work is outlined: (1) model compression techniques such as quantization and pruning to fit inference on even smaller edge devices; (2) integration of Fast DDS with kernel‑bypass technologies (XDP/DPDK) to further shrink latency; (3) expansion to multi‑modal data (e.g., clinical metadata) and multi‑hospital federated learning; and (4) field trials in actual remote clinics to assess usability and clinical impact.
In conclusion, the study demonstrates that a carefully engineered combination of a proven deep‑learning classifier and a standards‑based real‑time middleware can deliver effective, low‑latency diagnostic assistance in bandwidth‑limited, resource‑constrained healthcare environments, paving the way for scalable AI‑enabled telemedicine solutions in underserved regions.
Comments & Academic Discussion
Loading comments...
Leave a Comment