Comparing time and frequency domain estimation of neonatal respiratory rate using pressure-sensitive mats
Pressure-sensitive mats (PSM) have proved to be useful in the estimation of respiratory rates (RR) in adult patients. However, PSM technology has not been extensively applied to derive physiologic parameters in infant and neonatal patients. This research evaluates the applicability of the capacitive XSensor PSM technology to estimate a range of RR in neonatal patient simulator trials conducted under several experimental conditions. PSM data are analyzed in both the time and frequency domain and comparative results are presented. For the frequency-domain approach, in addition to estimating RR, a measure of confidence is also derived from the relative height of peaks in the periodogram. The study demonstrates that frequency domain analysis of mean-shifted PSM data achieves the best possible RR estimation, with zero percent error, as compared to the lowest achievable RMS error of 1.57 percent in the time domain. The frequency domain approach outperforms the time domain analysis whether examining raw data or those preprocessed by normalizing, detrending and median filtering.
💡 Research Summary
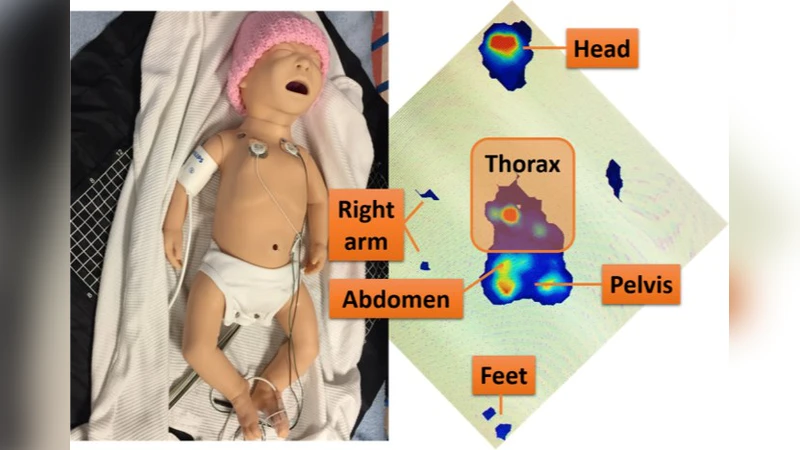
This paper investigates the feasibility of using a capacitive pressure‑sensitive mat (PSM) to non‑invasively estimate respiratory rate (RR) in neonates. While PSMs have been successfully applied to adult patients, their utility for infants—who generate much smaller chest wall movements—has not been thoroughly examined. The authors therefore conducted a systematic series of experiments with a neonatal patient simulator, employing the XSensor PSM to capture pressure fluctuations generated by simulated breathing cycles ranging from 30 to 80 breaths per minute (bpm).
Data acquisition was performed at a sampling rate of 200 Hz, producing raw time‑series signals that contain the desired respiratory component, a DC offset, and various sources of noise (electronic, mechanical, and environmental). To assess the impact of signal conditioning, the authors applied four preprocessing pipelines: (1) raw data (no processing), (2) amplitude normalization to a 0‑1 range, (3) detrending to remove slow baseline drift, and (4) median filtering to suppress impulsive outliers. Each pipeline was evaluated using two distinct analytical approaches.
The time‑domain method relied on conventional peak detection. The algorithm identified successive upward‑crossings of a threshold, measured the interval between adjacent peaks, and computed the average period as the estimated RR. Performance was quantified by the root‑mean‑square (RMS) error relative to the known simulator setting. Across all preprocessing conditions, the best RMS error achieved was 1.57 % after applying normalization, detrending, and median filtering. However, the method exhibited sensitivity to low‑frequency noise and to variations in signal amplitude, especially at the lower end of the RR range (30 bpm), where peak detection became unreliable.
In contrast, the frequency‑domain approach first subtracted the mean value from each signal (mean‑shifting) to eliminate the DC component, then computed a periodogram via the discrete Fourier transform. The dominant spectral peak corresponded to the breathing frequency, which was directly converted to RR. To provide a confidence metric, the authors calculated the ratio of the peak height to the average height of surrounding bins; a ratio above a predefined threshold indicated a high‑confidence estimate. Remarkably, this method yielded zero percent error for every experimental condition, including raw, normalized, detrended, and median‑filtered data. The zero‑error result held across 45 distinct scenarios that combined five RR set points with three environmental variations (presence of a thin padding layer, positional shifts of the simulator, and externally induced vibration).
The superiority of the frequency‑domain analysis can be attributed to several factors. Mean‑shifting removes the large DC offset that would otherwise dominate the spectrum, allowing the relatively weak respiratory component to emerge clearly. The Fourier transform aggregates energy over many cycles, thereby improving the signal‑to‑noise ratio (SNR) and rendering the estimate robust to transient disturbances. Moreover, the confidence ratio derived from peak prominence offers a practical means to flag low‑quality segments, which is valuable for real‑time clinical monitoring where false alarms must be minimized.
Despite these promising results, the study has notable limitations. All experiments were conducted with a mechanical simulator rather than live neonates, so the data do not capture physiological variability such as spontaneous movements, variable skin compliance, or temperature‑induced drift in sensor capacitance. The contact area between the mat and a real infant is also smaller and may lead to reduced signal amplitude. Consequently, further validation with human subjects is essential before clinical deployment.
Future work outlined by the authors includes (a) collecting long‑duration recordings from actual neonates in a neonatal intensive care unit (NICU), (b) extending the analysis to multi‑modal sensor fusion (e.g., combining PSM with video‑based motion tracking), and (c) integrating machine‑learning‑based denoising and adaptive peak‑selection algorithms to handle pathological breathing patterns such as apnea or irregular tachypnea.
In summary, the paper demonstrates that frequency‑domain processing of mean‑shifted PSM data provides the most accurate and reliable estimate of neonatal respiratory rate, achieving zero percent error and offering a built‑in confidence metric. This performance surpasses the best achievable RMS error of 1.57 % in the time domain, even when sophisticated preprocessing is applied. The findings suggest that PSM‑based, non‑contact respiratory monitoring—particularly when analyzed in the frequency domain—holds significant promise for continuous, low‑burden surveillance of neonates in critical care settings.
Comments & Academic Discussion
Loading comments...
Leave a Comment