Toward an improved BCI for damaged CNS-tissue patient using EEG-signal processing approach
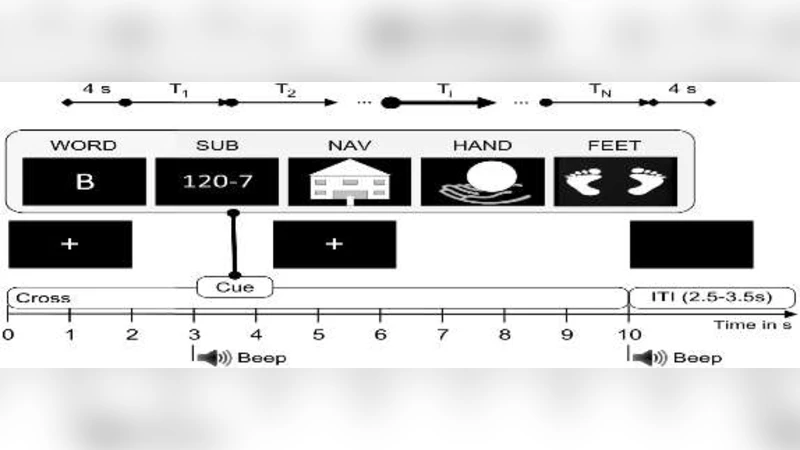
This article examined brain signals of people with disabilities using various signal processing methods to achieve the desired accuracy for utilizing brain-computer interfaces (BCI). EEG signals resulted from 5 mental tasks of word association (WORD), Mental subtraction (SUB), spatial navigation (NAV), right-hand motor imagery (HAND), and feet motor imagery (FEET) of 9 people with central nervous system (CNS) tissue damage were used as input. In processing this data, Butterworth band-pass filter (8-30 Hz) was used in the preprocessing, and CSP, TRCSP, FBCSP methods were used in feature extraction, and LDA, KNN, linear and nonlinear SVM were used in classification stages. The training and testing process was repeated up to 100 times, and the random subsampling method was used to select the training and test data. Mean accuracy in 100 replications was reported as final accuracy. The classification results of two classes of 5 mental tasks on the data of 9 people with central nerve damage showed that the combination of FBCSP with KNN classifier has the highest accuracy of 69+-1.1 which belongs to the two classes of word association and feet motor imagery. The study of different feature extraction methods and classification indicates that the proper feature selection method and especially classifier is crucial in accuracy rate. Furthermore, it is necessary to pay attention to successful signal processing methods in designing a brain-computer interface to use in people with central nervous system.
💡 Research Summary
The paper investigates the feasibility of building a brain‑computer interface (BCI) for patients with central nervous system (CNS) damage by systematically comparing several EEG signal‑processing pipelines. Nine participants with documented CNS injury performed five distinct mental tasks: word association (WORD), mental subtraction (SUB), spatial navigation (NAV), right‑hand motor imagery (HAND), and feet motor imagery (FEET). EEG recordings were first band‑pass filtered between 8 Hz and 30 Hz using a fourth‑order Butterworth filter, a conventional choice that preserves the alpha and beta bands while attenuating low‑frequency drift and high‑frequency noise that are often amplified in clinical populations.
Three feature‑extraction strategies were evaluated. The classic Common Spatial Pattern (CSP) algorithm extracts spatial filters that maximize variance differences between two classes. Temporal‑Recursive CSP (TRCSP) extends CSP into the time‑frequency domain, attempting to capture dynamic changes in spectral content. Filter‑Bank CSP (FBCSP) decomposes the signal into several narrow sub‑bands (e.g., 8‑12 Hz, 12‑16 Hz, 16‑20 Hz, 20‑24 Hz, 24‑30 Hz), applies CSP to each band, and concatenates the resulting features, thereby exploiting frequency‑specific discriminative information. The authors hypothesized that the heterogeneous nature of EEG in CNS‑damaged brains would benefit from the multi‑band approach.
Four classifiers were tested: Linear Discriminant Analysis (LDA), k‑Nearest Neighbors (KNN), linear Support Vector Machine (SVM), and nonlinear SVM (RBF kernel). LDA provides a fast, linear decision surface; KNN is a non‑parametric, distance‑based method that can model complex boundaries; SVM variants offer margin‑maximizing hyperplanes with optional kernel‑induced nonlinearity. The classification pipeline was evaluated using a random subsampling (Monte‑Carlo) scheme: for each of 100 repetitions, the dataset was randomly split into training and test sets, the model was trained, and accuracy on the held‑out test set was recorded. The final performance metric is the mean accuracy across the 100 repetitions, accompanied by the standard deviation.
Because the five tasks constitute a multi‑class problem, the authors reduced the analysis to binary discrimination between pairs of classes. The most notable result emerged from the WORD vs. FEET pair: the combination of FBCSP for feature extraction and KNN for classification achieved a mean accuracy of 69 ± 1.1 %. This was the highest reported performance among all feature‑classifier pairings. Other combinations, such as CSP‑LDA or TRCSP‑linear SVM, yielded accuracies in the 55–62 % range, indicating that neither a single‑band CSP nor a purely linear classifier could capture the discriminative patterns present in this clinical EEG dataset.
The study underscores several key insights. First, the choice of feature extraction method has a pronounced impact on BCI performance for CNS‑damaged users; multi‑band CSP appears to harness frequency‑specific information that single‑band approaches miss. Second, classifier selection is equally critical; a simple, non‑parametric KNN outperformed more sophisticated linear and kernel‑based SVMs, likely because the limited training data and the non‑stationary nature of the signals favor a method that relies on local similarity rather than global hyperplane separation. Third, the repeated random subsampling protocol provides a robust estimate of generalization performance, mitigating over‑optimistic results that can arise from a single train‑test split.
Nevertheless, the work has notable limitations. The sample size (n = 9) is modest, restricting statistical power and the ability to generalize findings to the broader CNS‑injured population. Moreover, the binary classification focus sidesteps the practical challenge of distinguishing all five mental tasks simultaneously, which is essential for real‑world BCI applications. The reported 69 % accuracy, while the best among the tested configurations, remains below the typical threshold (~80 %) required for reliable assistive communication. Computational complexity was not addressed; while KNN is simple to implement, its inference cost scales with the size of the training set, which could hinder real‑time deployment.
Future research directions suggested by the authors—and reinforced by this analysis—include expanding the participant pool to encompass diverse injury etiologies (stroke, traumatic brain injury, neurodegenerative conditions), evaluating full multi‑class classification performance, and integrating adaptive or online learning schemes to accommodate intra‑session variability. Additionally, comparing the current pipeline with deep learning approaches (e.g., convolutional neural networks that learn spatial‑temporal filters directly from raw EEG) could reveal whether end‑to‑end models can surpass hand‑crafted feature methods in this clinical context. Finally, a systematic assessment of latency, power consumption, and user‑centric metrics (fatigue, comfort) will be essential for translating these findings into a usable BCI system for patients with CNS damage.