Fallopian tube anatomy predicts pregnancy and pregnancy outcomes after tubal reversal surgery
We conducted this study to determine whether fallopian tube anatomy can predict the likelihood of pregnancy and pregnancy outcomes after tubal sterilization reversal. We built a flexible, non-parametric, multivariate model via generalized additive models to assess the effects of the following tubal parameters observed during tubal reparative surgery: tubal lengths; differences in tubal segment location, and diameters at the anastomosis sites; and, fibrosis of the tubal muscularis. In this study population, age and tubal length - in that order - were the primary factors predicting the likelihood of pregnancy. For pregnancy outcomes, tubal length was the most influential predictor of birth and ectopic pregnancy, while age was the primary predictor of miscarriage. Segment location and diameters contributed slightly to the odds of miscarriage and ectopic pregnancy. Tubal muscularis fibrosis had a little apparent effect. This study is the first to show that a statistical learning predictive model based on fallopian tube anatomy can predict pregnancy and pregnancy outcome probabilities after tubal reversal surgery.
💡 Research Summary
This study investigates whether anatomical characteristics of the fallopian tubes observed during tubal reversal surgery can predict both the likelihood of achieving pregnancy and subsequent pregnancy outcomes (live birth, miscarriage, ectopic pregnancy, or ongoing pregnancy). Using a prospective observational cohort from a single outpatient surgical center in Chapel Hill, North Carolina, the authors identified 5,682 women who underwent bilateral tubotubal anastomosis between January 2000 and June 2013, had complete anatomical data for both tubes, and at least one year of postoperative follow‑up.
For each patient, five predictors were extracted: (1) age at surgery, (2) total length of the re‑anastomosed tube, (3) segment‑position difference (SPD) between the two joined segments (coded 0–3), (4) diameter difference at the anastomosis (categorized as similar, somewhat dissimilar, or dissimilar), and (5) degree of muscularis fibrosis (none, mild, moderate, severe). Because the specific tube (left or right) that ultimately contributed to a pregnancy is unknown, the authors simulated this uncertainty by randomly assigning each woman either the left‑ or right‑tube data with a 50 % probability, effectively treating the choice as a Bernoulli trial.
Two generalized additive models (GAMs) were fitted using the mgcv package in R. The first model addressed pregnancy occurrence as a binary outcome with a logit link, incorporating smooth cubic spline terms for age and tube length and categorical terms for SPD, diameter difference, and fibrosis. The second model treated pregnancy outcome as a multinomial response (birth, ongoing, miscarriage, ectopic) and used an analogous GAM structure. Model performance was evaluated with cross‑entropy loss, Akaike Information Criterion (AIC), and Bayesian Information Criterion (BIC); partial dependence plots (PDPs) were generated to visualize marginal effects.
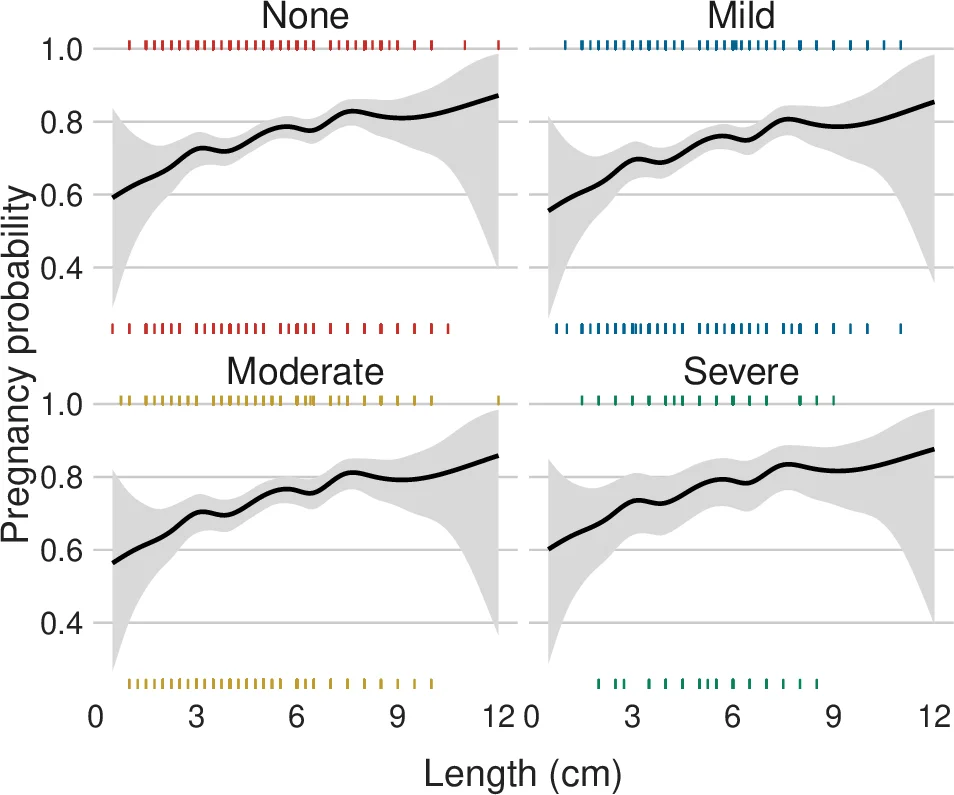
Key findings: (i) Age emerged as the dominant negative predictor of pregnancy across all anatomical sub‑groups; the probability of conception declined steadily with age and dropped sharply after approximately 35 years. (ii) Tubal length was the second most important predictor; longer tubes (≥5 cm) were associated with higher conception rates and markedly increased odds of live birth, while shorter tubes were linked to higher risks of miscarriage and ectopic pregnancy. (iii) Segment‑position differences and diameter mismatches contributed modestly, primarily increasing the odds of miscarriage and ectopic pregnancy when differences were larger. (iv) Fibrosis showed little to no effect on either pregnancy likelihood or outcome.
The authors conclude that incorporating intra‑operative anatomical measurements—particularly tube length—into predictive models substantially improves the ability to counsel women about their reproductive prospects after tubal reversal, beyond the traditional reliance on age and sterilization method alone. The use of GAMs allowed the capture of non‑linear relationships (e.g., the steep age‑related decline) and provided interpretable visualizations of each predictor’s marginal impact. Limitations include the random assignment of left/right tube data, which may not reflect the true contributing tube, and the single‑center design, which could limit generalizability. Future work should aim to identify the actual tube responsible for conception, explore interaction effects among anatomical variables, and validate the model in external cohorts.
Comments & Academic Discussion
Loading comments...
Leave a Comment