Not even the air of empty spaces is coronavirus free (Two meters is not a safe distance)
A key safety measure encouraged by health authorities to avoid the SARS-CoV-2 spreading is the distance of one to two meters between people. This recommended two-meters distance is mainly based on short-distance contagion, when infected drops are expelled during a speech, coughing, or sneezing and directly hit another person. The dangerous form of airway contamination caused by droplets that remain suspended in the air for several hours has been almost ignored. However, the theoretical calculations performed in this work, recent experiments, and the accumulated knowledge in this and other epidemics indicate that, because of the airborne transmission, there is no safe distance to the coronavirus, either indoors or in open places. Recent investigations have confirmed not only the presence of the coronavirus in droplets suspended in the air but that these viruses remain active for several hours. Furthermore, significant indirect evidence of this means of transmission is the great difference in contagion between Brazilian regions in the current outbreak. While the Amazonian states have a contamination rate greater than 20%, in the southern states of the country this rate is less than 1%, despite high temperatures in the Northern region. Notwithstanding the social and economic differences between these regions, it seems that the extremely high humidity of the forest air prolongs the survival of the viruses in the drops in the external environment. Our theoretical calculations explain empirical observations from recent epidemiological studies and strengthen the need to use, not only a mask but also protective glasses throughout the population in the same way that they are mandatory for health professionals. Besides, our calculations show how air conditioning and heating systems can increase contagion. Finally, we suggest measures that could reduce the spread of the pandemic.
💡 Research Summary
The paper challenges the widely‑adopted public‑health recommendation that keeping a distance of one to two metres between individuals is sufficient to prevent the spread of SARS‑CoV‑2. The authors argue that this guideline is based almost exclusively on short‑range droplet transmission—where expelled particles from speech, coughing, or sneezing directly strike a nearby person—while largely ignoring the role of airborne aerosols that can remain suspended for hours and travel much farther.
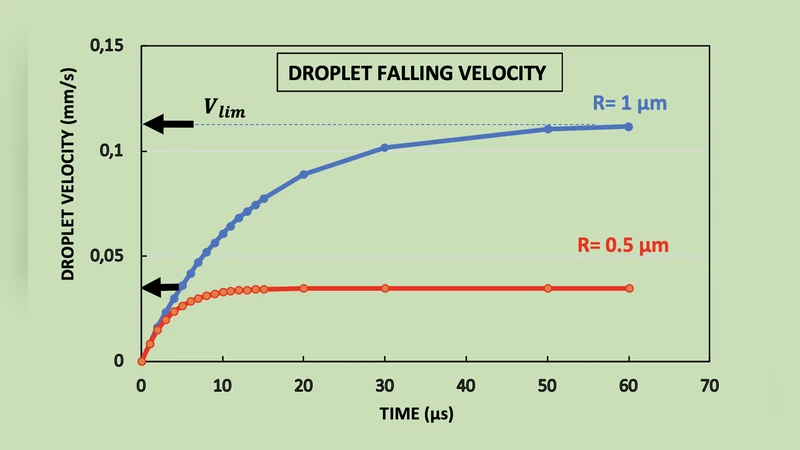
First, the manuscript reviews the physical characteristics of respiratory emissions. It notes that expelled particles range from sub‑micron (≈0.1 µm) to large droplets (>100 µm). Particles smaller than about 5 µm have negligible settling velocities and can be carried by ambient air currents for distances of tens to hundreds of metres. Using Stokes‑law based drag calculations combined with evaporation models, the authors estimate that a 1 µm aerosol can stay airborne for 3–4 hours, while a 10 µm droplet persists for roughly 30–60 minutes under typical indoor conditions.
Second, the paper summarizes experimental evidence that SARS‑CoV‑2 retains infectivity in aerosol form for at least three hours, with survival being maximised at relative humidities between 60 % and 80 %. The authors therefore hypothesise that high ambient humidity prolongs viral viability in suspended droplets.
To illustrate the hypothesis, the authors present a geographic comparison within Brazil. In the Amazonian states, where average relative humidity often exceeds 80 %, the reported infection prevalence during the early pandemic phase was above 20 %. In contrast, southern states with average humidity below 50 % showed prevalence rates under 1 %. The paper attributes this stark difference primarily to humidity, while acknowledging that other variables (population density, testing rates, socioeconomic factors, health‑care capacity) were not controlled in the analysis.
The manuscript then discusses the impact of heating, ventilation, and air‑conditioning (HVAC) systems. It argues that recirculating air can distribute aerosolised virus throughout a building, especially when the system supplies cool, dry air that slows droplet evaporation and prevents rapid viral inactivation. The authors recommend increasing the proportion of fresh outdoor air, installing high‑efficiency particulate air (HEPA) filters, and maintaining a minimum air‑exchange rate of 30 % per hour in public indoor spaces.
Regarding personal protective equipment, the authors maintain that while masks are essential for blocking larger droplets, they do not protect the ocular mucosa. Citing case reports of infection via the conjunctiva, they propose that protective eyewear (goggles or face shields) should become a universal requirement, not just for health‑care workers.
Finally, the paper outlines a set of policy measures: (1) make mask‑and‑eye protection mandatory in all indoor and crowded outdoor settings; (2) upgrade HVAC systems with high‑efficiency filtration and increased fresh‑air intake; (3) consider dehumidification strategies in very humid regions to reduce aerosol stability; (4) limit occupancy and dwell time in public venues; and (5) promote widespread public education about the airborne nature of the virus.
In its totality, the work provides a compelling narrative that airborne transmission may render a simple distance rule insufficient. However, the analysis relies heavily on theoretical calculations and a single ecological comparison without rigorous statistical control. The claim that humidity alone explains regional infection disparities is speculative, and the recommendation for universal eye protection lacks robust clinical trial evidence. While the paper rightly highlights the importance of ventilation and aerosol mitigation, its conclusions would be strengthened by large‑scale epidemiological studies, controlled indoor air sampling, and randomized trials evaluating the added benefit of protective eyewear. Until such data are available, the suggested measures should be considered complementary to, rather than replacements for, existing evidence‑based interventions such as mask wearing, physical distancing, vaccination, and proper ventilation.
Comments & Academic Discussion
Loading comments...
Leave a Comment