A low-cost real-time 3D imaging system for contactless asthma observation
Asthma is becoming a very serious problem with every passing day, especially in children. However, it is very difficult to detect this disorder in them, since the breathing motion of children tends to change when they reach an age of 6. This, thus makes it very difficult to monitor their respiratory state easily. In this paper, we present a cheap non-contact alternative to the current methods that are available. This is using a stereo camera, that captures a video of the patient breathing at a frame rate of 30Hz. For further processing, the captured video has to be rectified and converted into a point cloud. The obtained point clouds need to be aligned in order to have the output with respect to a common plane. They are then converted into a surface mesh. The depth is further estimated by subtracting every point cloud from the reference point cloud (the first frame). The output data, however, when plotted with respect to real time produces a very noisy plot. This is filtered by determining the signal frequency by taking the Fast Fourier Transform of the breathing signal. The system was tested under 4 different breathing conditions: deep, shallow and normal breathing and while coughing. On its success, it was tested with mixed breathing (combination of normal and shallow breathing) and was lastly compared with the output of the expensive 3dMD system. The comparison showed that using the stereo camera, we can reach to similar sensitivity for respiratory motion observation. The experimental results show that, the proposed method provides a major step towards development of low-cost home-based observation systems for asthma patients and care-givers.
💡 Research Summary
The paper presents a low‑cost, real‑time, contact‑less system for monitoring respiratory motion in children with asthma, using a single stereo camera. The authors argue that existing contact‑based methods (e.g., chest belts) are uncomfortable and can interfere with natural breathing, while single‑camera RGB approaches lack depth information and depend on ambient lighting. Their solution employs a passive USB‑3.0 stereo camera (≈75 €) that records synchronized left‑right video at 30 Hz and 480 × 1280 resolution.
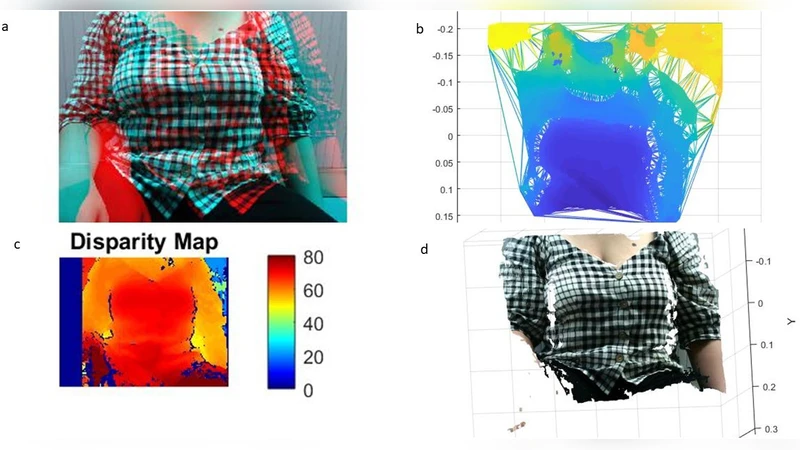
Calibration is performed with a 7 × 10 checkerboard (10 mm squares) captured from multiple viewpoints; MATLAB’s Stereo Calibration App provides intrinsic and extrinsic parameters, after which each frame is rectified to simplify correspondence search. Disparity maps are computed, filtered, and converted into 3D point clouds. Invalid points and various noise types (salt‑and‑pepper, quantization, white) are removed. To compare successive frames, the Iterative Closest Point (ICP) algorithm aligns every point cloud to the first frame, establishing a common coordinate system. The aligned clouds are meshed, and depth change is obtained by subtracting each frame’s depth from the reference frame, producing a raw breathing signal.
The raw signal is heavily contaminated, so the authors apply a Fast Fourier Transform (FFT) to identify the dominant breathing frequency and design a band‑pass filter that isolates the respiratory component while suppressing other frequencies. They note that the optimal frequency band varies with breathing type (deep, shallow, normal, coughing), indicating that a universal fixed band is not feasible.
Experiments were conducted with an adult volunteer performing four breathing patterns: deep, shallow, normal, and coughing, each recorded for about 30 seconds. The system’s sampling rate of 30 Hz proved essential; reducing it to 6.7 Hz dramatically increased noise. The authors also examined the effect of region‑of‑interest (ROI) selection. Using the whole chest area improved signal‑to‑noise ratio, whereas a tiny ROI (a single pixel) yielded a noisier FFT output and missed cycles when the subject switched breathing mechanisms mid‑recording.
The processed breathing signal is displayed in a MATLAB GUI, which also counts breaths per 30‑second interval and presents the count to the user. To validate accuracy, the authors compared their depth measurements with those from a commercial 3dMD system, considered a gold standard in medical 3D imaging. Using CloudCompare to analyze point clouds from both systems, they found the 3dMD measured a maximum chest expansion of 36.0661 mm (error ± 1.783 mm) while the stereo‑camera system measured 38.4005 mm (error ± 1.542 mm). The ~2 mm difference demonstrates that the low‑cost setup achieves comparable sensitivity. Potential sources of discrepancy include calibration errors, clothing thickness, and the choice of reference frame.
The authors conclude that their inexpensive, non‑intrusive system can reliably monitor respiratory motion, making it suitable for home‑based asthma management, especially for children whose symptoms may evolve with age. They acknowledge remaining challenges: automating the selection of the appropriate frequency band, ensuring robustness when the first frame is not at a neutral breathing phase, and extending validation to pediatric subjects. Future work may involve adaptive filtering, machine‑learning‑based pattern recognition, and integration with remote health platforms.
Overall, the study demonstrates that a modest stereo camera, combined with standard computer‑vision pipelines (calibration, rectification, disparity, ICP alignment, FFT filtering), can provide medically relevant respiratory metrics at a fraction of the cost of existing commercial systems.
Comments & Academic Discussion
Loading comments...
Leave a Comment