retina-VAE: Variationally Decoding the Spectrum of Macular Disease
In this paper, we seek a clinically-relevant latent code for representing the spectrum of macular disease. Towards this end, we construct retina-VAE, a variational autoencoder-based model that accepts a patient profile vector (pVec) as input. The pVe…
Authors: Stephen G. Odaibo
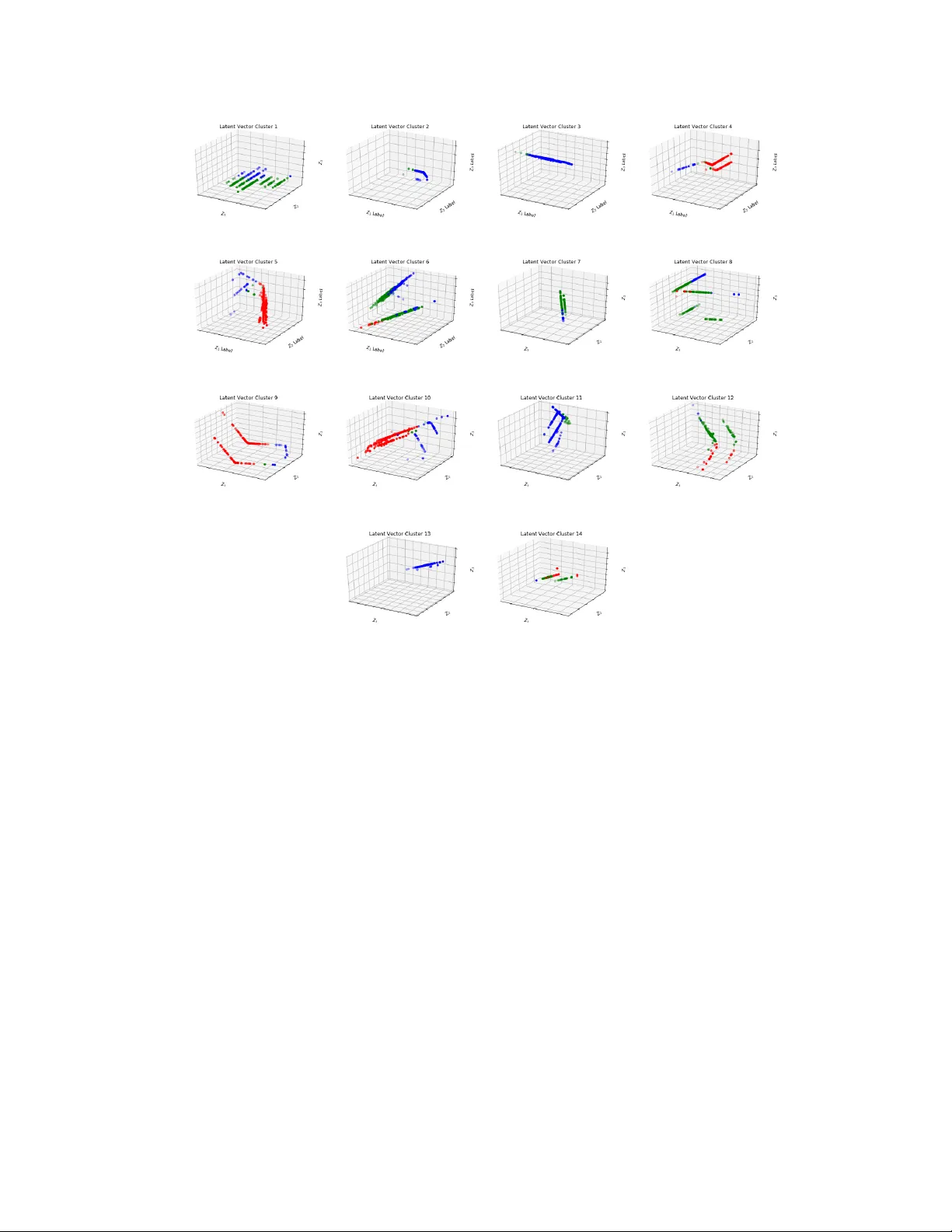
r etina-V AE: V ariationally Decoding the Spectrum of Macular Disease Stephen G. Odaibo ∗ (1) Department of Machine Learning Research RETIN A-AI Health, Inc. (2) Department of Head & Neck Surgery Ophthalmology Section MD Anderson Cancer Center stephen.odaibo@retina-ai.com Abstract In this paper , we seek a clinically-rele vant latent code for representing the spec- trum of macular disease. T ow ards this end, we construct retina-V AE, a variational autoencoder-based model that accepts a patient profile vector (pV ec) as input. The pV ec components include clinical exam findings and demographic information. W e ev aluate the model on a subspectrum of the retinal maculopathies, in particular , exudati ve age-related macular degeneration, central serous chorioretinopath y , and polypoidal choroidal v asculopathy . For these three maculopathies, a database of 3000 6-dimensional pV ecs (1000 each) was synthetically generated based on known disease statistics in the literature. The database was then used to train the V AE and generate latent vector representations. W e found training performance to be best for a 3-dimensional latent vector architecture compared to 2 or 4 dimensional latents. Additionally , for the 3D latent architecture, we discovered that the resulting latent vectors were strongly clustered spontaneously into one of 14 clusters. Kmeans was then used only to identify members of each cluster and to inspect cluster properties. These clusters suggest underlying disease subtypes which may potentially respond better or worse to particular pharmaceutical treatments such as anti-v ascular en- dothelial growth f actor v ariants. The retina-V AE framework will potentially yield new fundamental insights into the mechanisms and manifestations of disease. And will potentially facilitate the dev elopment of personalized pharmaceuticals and gene therapies. 1 Introduction In current clinical practice, physicians see patients and based on a combination of objecti ve and subjectiv e information gathered, make a diagnoses of the condition. The diagnosis is howev er typically based on a rigid and mut ually exclusi v e classification of the disease. This system is brittle as it does not tak e into account that most diseases manifest between and outside of these rigid classes, and it does not provide opportunity for personalized diagnosis and treatment. Increasingly as clinicians become more aware of the inadequacies of the current system, there is a concept of “Spectrum of disease. ” It recognizes that the genetic, metabolic, environmental, and demographic profile of a patient points to predilection for specific manifestations which may be better or less responsi ve to any particular treatment. In the case of the retinal maculopathies for instance, a prototypical one is age-related macular degeneration (ARMD), which in a certain subtype progresses into an exudati v e state which requires intra vireal injections with anti v ascular endothelial gro wth factor (anti-VEGF) ∗ Correspondence: RETIN A-AI Health, Inc. P .O.Box 20169, Houston TX Preprint. Under re view . (a) (b) Figure 1: (a) Normal retina (b) Retina with age-related macular degeneration showing large dif fuse soft confluent drusen (yellow dots) injections. In the absence of this treatment, patients will often go blind. It is kno wn to practicing retina specialists that there are multiple manifestations of this condition, simply based on the broad range of presentations and responses to treatment. Howe v er , this notion is yet to be rigorously quantified and described. For instance, certain patients with what would appear to be central serous chorioretinopathy , do progress to dev elop choroidal neo v ascular membranes and respond positively to intravitreal injections of anti-VEGF . Similarly , polypoidal choroidal v asculopathy is another related disease with clear distinctions from ARMD, that also requires intravitreal injections for treatment. In this paper , we sought out to develop a frame work for the study and characteization of this notion of a “spectrum of macular disease, ” a notion that if properly described, can potentially yield significant advances in the de v elopment of personalized pharmaceuticals and gene therapies. From a methodological standpoint, the notion of seeking latent codes that represent a data distribution is certainly not ne w . V arious techniques and efforts such as principal component analysisJolliffe (2011) and kmeans clusteringMacQueen et al. (1967); W agstaf f et al. (2001); Coates et al. (2011); Coates and Ng (2012) ha ve been ongoing for a while in the statistics community . W ithin machine learning, there has been some early w ork in adv ersarial generati ve modelingSchmidhuber (1992), and more recently , a great surge of interest since the entry of generative adv ersarial networks Goodfellow et al. (2014); Radford et al. (2015); Mirza and Osindero (2014). Another class, autoencoding algorithms generate a latent representation and then reconstruct the input data from the latent using the data itself as the labelLe et al. (2011); Hinton and Salakhutdinov (2006); Lee et al. (2009); V incent et al. (2010); Ngiam et al. (2011). These did not yield a continuous latent space, and as such were not truly generativ e in the sense of having capacity to generate meaningful (or interpretable) data for any point in the latent space. This was addressed by Kingma and W elling via v ariational autoencodersKingma et al. (2013), which is what we have adopted in retina-V AE. W e see variational inference as particularly suitable for the problem of discov ering latent features which hold diagnostic and therapeautic relev ance. There has been some related work using V AEs to determine rele vant latent representations for disease stratification. For instance, W ay et al used V AEs to extract a latent space from cancer transcriptomesW ay et al. (2017). Rampasek et al used V AEs to deduce latent space of drug response in cancer cell lines. And Cohen et al used an autoencoder to obtain a representation of in situ hybridization images.Cohen et al. (2017). No studies to date have yet been done on utilizing variational autoencoders to determine clinically rele v ant latent spaces for retinal disease diagnosis. 2 Background The retina is the sensory tissue in the back of the e ye. It contains the photoreceptors which absorb light and transmit a signal onwards to the primary visual corte x (area V1) via the optic nerve. Figure 1 (a) shows a normal retina. V arious diseases can affect the retina resulting in vision loss and blindness. One such disease is age-related macular degeneration (ARMD)V inding et al. (1989) which is the leading cause of blindness in people ov er the age of 50 in the United States. Figure 1 (b) sho ws the retina of a patient with ARMD. The condition often starts out in a “non-exudati ve” state and progresses with age into an “exudati ve” state, because of renegade blood vessels called choroidal neov ascular membranes which pathologically arise from the choroid, the v ascular layer underneath 2 the retina, and break through bruch’ s membrane and into the subretinal space where the y leak and cause vision loss. When such an exudativ e transformation occurs, to decrease vision loss and prev ent blindness intravitreal injections of anti-VEGF are required typically anywhere from monthly to once ev ery 3 months. Central serous chorioretinopathy (CSCR)Lie w et al. (2013); Castro-Correia et al. (1992) is another disease of the macular and associated central choroid. It typically occurs in men in their 30s to 40sCastro-Correia et al. (1992); Tsai et al. (2013) and has been associated with stress or steroid usage. T ypically , this condition resolv es on its o wn within a fe w weeks and does not require particular intervention, other than a caution to abstain from any steroid use such as in nasal sprays. In its more common form, CSCR is not thought of as being related to ARMD. Howe ver , in some instances, CSCR can become chronic and can de velop choroidal neo v ascular membranes requiring treatment with anti-VEGFs. This is typically termed “atypical CSCR” and is understood to be some where in the spectrum of ARMD. It is not currently understood why some patients with CSCR follo w a dif ferent prognostic course and end up requiring intravitreal injections potentially indefinitely , while most others hav e complete resolution of symptoms within weeks without ev er having a recurrence, and yet others hav e complete resolution within weeks, but then hav e recurrences periodically . V ariational substratification of the disease and discov ery of rele vant latent represenattion codes will lik ely help answer these open questions. Polypoidal choroidal vasculopathy (PCV) is another related condition, one in which polyps patholog- ically arise in the choroid. The polyps leak and can progressiv ely disrupt bruch’ s membrane, causing choroidal neov ascular membranes, subretinal hemorrhages (bleeds), and vision loss. The condition is often confused with exudati ve ARMD. Similarly to exudati ve ARMD, it responds positively to intravireal injections of anti-VEGF . This condition is most common in persons of Asian or African ancestry , but is increasingly being recognized in perons of European ancestry as well. PCV was not historically associated with drusen, ho we ver it is increasi ngly recognized that drusen-like deposits do occur in PCV patients. Such pattern is a recurrent theme undermining the traditional notion of singular ‘hallmark feature switches’ which can absolutely discriminate between diseases. As these once presumed ‘absolute discriminants’ are increasingly found with some, albeit lo wer , probability in the alternativ e diagnoses. This further underscores the need for probabilistic models which can distill clinically-rele vant latent representation codes, and variationally infer classes of disease for personalized treatment. In v ariational inference, the goal often is to determine a posterior distribution p ( z | x ) of a latent variable z giv en some data e vidence x . Ho we ver , determining this posterior distrib ution is typically computationally intractible, because according to Bayes, p ( z | x ) = Z z p ( x | z ) p ( z ) p ( x ) dz , (1) which is intractible because it in volv es computing the integral over the entire latent space z , and also typically because it requires knowledge or computation of the entire e vidence distribution p ( x ) . T o circumvent this intractibility problem one instead approximates the posterior with some other distribution q ( z | x ) in a manner that minimizes some similarity measure between the true posterior and the approximation, q . Here we use the Kullback-Leibler , D K L : D K L ( q ( z | x i ) || p ( z | x i )) = Z q ( z | x i ) log q ( z | x i ) p ( z | x i ) dz , (2) which when manipulated in the abov e yields the below log p ( x i ) = D K L ( q ( z | x i ) || p ( z | x i )) + E q ( z | x i ) [log p ( z , x i ) − log q ( z | x i )] . (3) Since D K L ≥ 0 , it follo ws that log p ( x i ) ≥ E q ( z | x i ) [log p ( z , x i ) − log q ( z | x i )] . (4) 3 (a) (b) (c) (d) (e) Figure 2: (a) Racial Distribution of Exudativ e Age-Related Macular Degeneration (ARMD) (b) Racial Distrib ution of Central Serous Chorioretinopath y (CSCR) (c) Racial Distribution of Polypoidal Choroidal V asculopathy (PCV) (d) Distribution of polyps, drusen, and subretinal hemorrhage in ARMD, CSR, and PCV (e) Age Distributions of e xudati ve ARMD, of CSCR, and of PCV . Therefore maximizing the log likelihood of the data is synonymous with maximizing the term on the right, the variational lo wer bound L . In the manner of Kingma et al Kingma et al. (2013), we utilize the variational lo wer bound as the loss function of our V AE. It can be reexpressed as: L = E q ( z | x i ) [log p ( z , x i ) − log q ( z | x i )] = Z z q ( z | x i ) [log p ( z , x i ) − log q ( z | x i )] dz (5) L = Z z q ( z | x i ) log p ( z , x i ) q ( z | x i ) dz = Z z q ( z | x i ) log p ( x i | z ) p ( z ) q ( z | x i ) dz (6) L = Z z q ( z | x i ) log p ( z ) q ( z | x i ) dz + Z z q ( z | x i ) log p ( x i | z ) dz (7) L = − D K L ( q ( z | x i ) || p ( z )) + E q ( z | x i ) [log p ( x i | z )] (8) Choosing a gaussian latent prior and a gaussian approximate posterior yields a closed form for the D K L term. The resulting loss function is then: L = − 1 2 J X j =1 1 + log( σ 2 j ) − µ 2 j − σ 2 j + 1 L L X l =1 E q ( z | x i ) h log p ( x i | z ( i,l ) ) i (9) where J is the dimension of the latent, σ j and µ j are parameters of the approximate posterior, q , and L is the number of samples stochastically drawn utilizing the reparametrization trickKingma et al. (2013). 3 Methods Three thousand patient profile vectors (pV ec) were generated based on literature on the epidemiology of the three maculopathies under study . Mean values and distribution information was obtained, distribution models b uilt, and then sampling carried out on the distrib utions. The pV ec consisted of the following 6 components: race, age, presence or absence of polyps, presence or absence of drusen or drusen-like deposits, presence or absence of subretinal hemorrhage (SRH), and sex. The random variables polyps, drusen, SRH, and se x had v alues of either 0 or 1. The race categories were asian, black, caucasian, hispanic, and other . The age random variable w as continuous, assuming v alues in the positiv e reals. 4 Figure 3: T raining Spectral-V AE with 2, 3, and 4 dimensional latent Figure 4: Composite Latent V ector Map Data Model For the data model, it was noted that CSCR has a median age of about 36 to 39 yearsCastro-Correia et al. (1992); Tsai et al. (2013). Hence for the CSCR age distribution model, we used a mean age of 39 years and a variance of 60. The mean age of patients af fected with PCV varied by study between 55 and 68 years Sho et al. (2003); Y annuzzi et al. (2012). Hence for the PCV age distribution model we used a mean age of 60 years and a variance of 40. The av erage age of patients with exudativ e (a) (b) (c) (d) Figure 5: (a) 3D latent vector space of exudati v e ARMD (b) 3D latent vector space of CSCR (c) 3D latent vector space of PCV (d) 3D latent vector space composite of e xudativ e ARMD, CSCR, and PCV 5 (a) (b) (c) (d) (e) (f) (g) (h) (i) (j) (k) (l) (m) (n) Figure 6: (a) Cluster 1 (b) Cluster 2 (c) Cluster 3 (d) Cluster 4 (e) Cluster 5 (f) Cluster 6 (g) Cluster 7 (h) Cluster 8 (i) Cluster 9 (j) Cluster 10 (k) Cluster 11 (l) Cluster 12 (m) Cluster 13 (n) Cluster 14 ARMD is about 80 years Jonas et al. (2003). Hence for exudativ e ARMD we used a mean age of 80 years and a variance of 80 in the data model. Figure 2 (e) shows age distribution of exudati v e ARMD, of CSCR, and of PCV used in our data model. Notably , exudativ e ARMD is most common amongst asians and caucasians and least common amongst blacks and hispanics Friedman et al. (1999); Kawasaki et al. (2010); V anderbeek et al (2011); Klein et al. (2006). Figure 2 (a) shows the racial distribution of exudati ve ARMD used in our data model. PCV is notably more common in people of Asian and African descent than in other racial groups Ciardella et al. (2004); Imamura et al. (2010), while CSCR is most common in asians, caucasians, and hispanics, and is relati vely rare in blacks Liew et al. (2013); Desai et al. (2003); Ahlers et al. (2009); Lin et al. (2016). Figures 2 (b) and (c) respectiv ely show the racial distribution of CSCR and of PCV used in our data model. In exudati ve ARMD, CSCR, and PCV , we respectiv ely used [0.39, 0.01, 0.5, 0.05,0.05], [0.33, 0.05, 0.32, 0.25, 0.05], and [0.4, 0.3, 0.10, 0.18, 0.02] as the categorical distributions amongst asians, blacks, caucasians, hispanics, and other races respectively . Drusen and drusen-like deposits have been observed in up to one third of patients with PCV Lafaut et al. (2000); Iwama et al. (2008). In our model we use 28% coincidence of drusen and PCV . Drusen or drusen-like deposits are kno wn to occur in CSCR Schatz et al. (1992); Chumbley et al. (1974) ev en though this is not a common occurence. W e model with 10% drusen or drusen-like occurence conincident with CSCR. About one third of patients with PCV were found to hav e large subretinal hemorrhage in one study Byeon et al. (2008). No definite sex predilection has been established for PCV Y annuzzi et al. (1999). Neither has there been any definite sex predilection established for e xudativ e ARMD V inding et al. (1989). Of note, for exudati ve ARMD a fe w studies ha ve noted some potentially race-specific se x predilection in either directionMaruko et al. (2007); Rudnicka et al. (2012), but nothing definite across the board. In our data model we used a uniform bernouli distrib ution for sex of PCV and exudativ e ARMD patients. 6 T able 1: Cluster characteristics ID Size Race Age Polyps Drusen SRH Sex 1 249 [249,0,0,0,0] [26,56,86] [249,0] [189,60] [68,181] [249,0] 2 198 [0,35,163,0,0] [23,39,70] [0,198] [0,198] [8,190] [198,0] 3 298 [0,8,229,35,0] [23,79,104] [0,298] [298,0] [57,241] [0,298] 4 220 [220,0,0,0,0] [24,79,105] [0,220] [220,0] [41,179] [220,0] 5 339 [0,141,78,104,16] [21,60,104] [339,0] [112,227] [101,238] [0,339] 6 225 [225,0,0,0,0] [30,61,92] [225,0] [71,154] [66,159] [0,225] 7 203 [0,129,74,0,0] [20,57,78] [203,0] [37,166] [55,148] [203,0] 8 186 [186,0,0,0,0] [30,78,107] [0,186] [186,0] [32,154] [0,186] 9 348 [0,11,268,43,26] [22,79,106] [0,348] [348,0] [54,294] [348,0] 10 154 [0,17,60,61,16] [14,40,75] [0,154] [0,154] [8,146] [0,154] 11 165 [165,0,0,0,0] [22,40,75] [0,165] [0,165] [7,158] [165,0] 12 69 [69,0,0,0,0] [22,39,59] [0,69] [0,69] [4,65] [0,69] 13 195 [0,0,36,141,18] [25,60,91] [195,0] [77,118] [61,134] [195,0] 14 151 [0,0,0,134,17] [18,39,63] [0,151] [0,151] [11,140] [151,0] T able 2: The ‘Size’ col is number of patients in cluster . ‘Race’ col sho ws race distribution with notation: [Asian, Black, Caucasian, Hispanic, Other]. ‘ Age’ column sho ws the age distribution as [min age, median age, max age]. ‘Polyps, ’ ‘Drusen, ’ and ‘SRH’ cols sho w respecti ve distrib utions as [number with, number without]. And ‘Sex’ col sho ws sex distribution as [number male, number female]. In CSCR, there is a significant male preponderence ranging anywhere from 1:3 to 1:7 Roberts et al. (2016); Kitzmann et al. (2008). Our dataset has been made publicly av ailable for do wnload at https://github .com/V eryV eryGoodNe ws/retina-V AE. Model Architectur e The V AE was implemented in K eras using the loss function described in Equation 9 abov e. The model architecture’ s encoder part consisted on 6-dimensional input vector , one hidden layer of size 512, and latent vectors of varying dimensions (2, 3, and 4) were set in experiment runs. For the encoder network, a r eLu was used as the acti v ation function of the hidden layer , and a linear activ ation function was used in the output. For the decoder network, a r eLu was used for the activ ation function of the hidden layer, while a sigmoid was used in the output layer . The decoder part of the model also consisted of a single hidden layer of size 512 and a 6 dimensional output. Training was done on an NVIDIA T esla V100 GPU with 16 GB RAM. And the number of iterations on the V AE was set to 1000 epochs. The reparametrization trickKingma et al. (2013) was utilized for the stochastic sampling of the latent vector during training. The loss function was plotted to monitor training. The code is av ailable for do wnload at https://github .com/V eryV eryGoodNews/retina-V AE. 4 Experiments & Results After training the V AE, the encoder network was detached such that the latent vector , z was encoder output. Inference was then run on this trained encoder to determine the latent vectors that corresponded to each pV ec vector in the training set. The latent vectors were plotted in the 3D latent case and 14 spontaneously formed clusters were visually observed as shown in Figure 5. Upon observation of these 14 clusters, kmeans w as run with a cluster size set to 14, so as to identify the members of the individual clusters. The ov erlay of latent vectors of all 3 maculopathies under study is shown in Figure 5 (d). Notably , 8 of the 14 clusters were found to contain representati ves from all 3 maculopathies under study . Those 8 are clusters 4, 5, 6, 8, 9, 10, 12, and 14. On the other hand, 6 of the 14 clusters were found to contain representativ es from only CSCR and PCV . Those 6 clusters are clusters 1, 2, 3, 7, 11, and 13. The sizes of the clusters varied as sho wn in T able 1. The ‘ID’ column shows the cluster ID, i.e cluster 1 has ID of 1. The ‘Size’ column shows number of patients in the cluster . The ‘Race’ column sho ws the race distribution in the cluster, and we hav e used notation [Asian, Black, Caucasian, Hispanic, Other]. The ‘ Age’ column shows the age distribution of the 7 cluster , sho wn as [min age, median age, max age]. The ‘Polyps’ column shows the polyps distribution of patients in the cluster, shown as [number with, number without]. The ‘Drusen’ column shows the ‘drusen’ distribution of patients in the cluster , shown as [number with, number without]. The ‘SRH’ column sho ws the subretinal hemorrhage distrib ution in the cluster , shown as [number with, number without]. And the ‘Sex’ column sho ws the sex distrib ution in the cluster , sho wn as [number male, number female]. Interestingly , the polyps and sex attrib utes were not mixed between clusters in the sense that for an y giv en cluster , the patients in the cluster either all had polyps or none of them had polyps; also, they were either all male or all female. Also interesting was the number of clusters which had all Asians and no other races. Those clusters are 1, 4, 6, 8, 11, and 12. No other races were the sole occupants of any cluster . Clusters 2, 12, and 14 had the lowest median ages of 39. Clusters 10 and 11 also had young median ages of 40. Clusters 3, 4, and 9 had the oldest median ages of 79, and cluster 8 was close with a median age of 78. Subretinal hemorrhage was the only categorical random v ariable that was completely mixed amongst the clusters, i.e. all clusters had some b ut not all patients with SRH. 5 Discussion The determination of clinically-relev ant latent codes holds the key to personalized medicine, and represents a critical step in that direction. It is interesting to ask how retina-V AE mechanistically went about grouping the pV ecs into these 14 classes. In statistical machine learning, dimensionality reduction is often presented as a process in which irrelev ant information is discarded. Ho we ver , our result here makes it apparent that dimensionality reduction can be an intelligent and more ef ficient rearrangement of information to fit into smaller dimensions. In this sense, one can think of the 14 clusters as representing an additional coordinate in the address space of the disease representation. For instance, such that when the decoder network “reads” a latent vector as arising from cluster 4 and kno ws to reconstruct that pV ec as being of the Asian race and male se x. Ho we ver , there are 14 spontaneous clusters yet only 4 or less of any gi ven attrib ute in the pV ec. Therefore, clearly as shown in T able 1, most clusters have a mixture of multiple dif ferent categories of an y giv en random variable. And these clusters are lik ely to hav e biological rele v ance and hold insights into the mechanisms of macular disease. The concept of dimensionality reduction such as going from a 6 dimensional pV ec to a 3D latent space is clinically appealing as it agrees with our intuition and clinical practice. It agrees with the notion that common pathophysiology and therefore common pharmacology connects and determines diseases in a spectrum. This concept of a spectrum of diseases is what we hav e set out here to decode for the maculopathies. Notably , all three of the maculopathies under study ha ve forms or states that require treatment with anti-VEGF drugs. Exudati ve ARMD and exudativ e PCV are treated with anti-VEGF in common and standard clinical practice, while atypical CSCR is a less common state often considered (or confused with) a v ariant of e xudativ e ARMD. All three conditions pathophysiologically in volv e or can progress to wards a disruption of Bruch’ s membrane and the subsequent formation of a choroidal neov ascular membrane. Once in this state, all three of these maculopathies respond positi vely to intra vitreal injection of anti-VEGF . This all suggests common physiological pathways which con v er ge under certain circumstances. As sho wn in Figure 6, within each of the 14 clusters, the indi vidual maculopathies are visually and computationally separable. Thus suggesting a multidimensional spectrum that could yield fundamen- tal insights about which patients will respond better or worse to what drugs. And consequently , about how to de v elop the best drugs. 6 Conclusion W e hav e introduced, retina-V AE, a novel application of v ariational autoencoders to wards determining a clinically relev ant latent space for exudati ve macular de generation and related conditions which require treatment with anti-VEGF agents. The latent vectors spontaneously formed into 14 clinically- relev ant clusters which are candidates for further disease characterization, personalized intervention, and optimal pharmaceutical dev elopment. 8 7 Future W ork The authors plan to further characterize and study the 14 clusters which formed spontaneously in retina-V AE. A clinical study will be conducted in which patients at our health center will be prospectiv ely classified into one of the 14 clusters by running inference using the trained retina-V AE model. These patients will then be followed to assess their phenotypic characteristics such as disease course, response to anti-VEGF treatment, injection interv al, genetic profile, co-morbidities, f amily history , and environmental exposures. This information could then potentially be used to provide treatment recommendations to optimize patient outcomes and to facilitate ne w drug de velopment. Acknowledgments The author thanks Google Cloud for providing the compute resources used in the e xperiments. References Castro-Correia J, Coutinho MF , Rosas V , Maia J. Long-term follow-up of central serous retinopathy in 150 patients. Documenta Ophthalmologica. 1992 Dec 1;81(4):379-86. Tsai DC, Chen SJ, Huang CC, Chou P , Chung CM, Huang PH, Lin SJ, Chen JW , Chen TJ, Leu HB, Chan WL. Epidemiology of idiopathic central serous chorioretinopathy in T aiwan, 2001–2006: a population-based study . PLoS One. 2013 Jun 24;8(6):e66858. Sho K, T akahashi K, Y amada H, W ada M, Nagai Y , Otsuji T , Nishikawa M, Mitsuma Y , Y amazaki Y , Mat- sumura M, Uyama M. Polypoidal choroidal vasculopathy: incidence, demographic features, and clinical characteristics. Archiv es of Ophthalmology . 2003 Oct 1;121(10):1392-6. Y annuzzi LA, Sorenson J, Spaide RF , Lipson B. Idiopathic polypoidal choroidal v asculopathy (IPCV). Retina. 2012 Feb 1;32:1-8. Jonas JB, Kreissig I, Hugger P , Sauder G, P anda-Jonas S, Degenring R. Intravitreal triamcinolone acetonide for exudati ve age related macular de generation. British Journal of Ophthalmology . 2003 Apr 1;87(4):462-8. Friedman DS, Katz J, Bressler NM, Rahmani B, Tielsch JM. Racial dif ferences in the prev alence of age-related macular degeneration: the Baltimore Eye Survey . Ophthalmology . 1999 Jun 1;106(6):1049-55. Kawasaki R, Y asuda M, Song SJ, Chen SJ, Jonas JB, W ang JJ, Mitchell P , W ong TY . The prev alence of age- related macular degeneration in Asians: a systematic revie w and meta-analysis. Ophthalmology . 2010 May 1;117(5):921-7. V anderbeek BL, Zacks DN, T alw ar N, Nan B, Musch DC, Stein JD. Racial dif ferences in age-related macular degeneration rates in the United States: a longitudinal analysis of a managed care network. American journal of ophthalmology . 2011 Aug 1;152(2):273-82. Ciardella AP , Donsoff IM, Huang SJ, Costa DL, Y annuzzi LA. Polypoidal choroidal vasculopath y . Survey of ophthalmology . 2004 Jan 1;49(1):25-37. Imamura Y , Engelbert M, Iida T , Freund KB, Y annuzzi LA. Polypoidal choroidal v asculopathy: a revie w . Survey of ophthalmology . 2010 Nov 1;55(6):501-15. Liew G, Quin G, Gillies M, Fraser-Bell S. Central serous chorioretinopathy: a revie w of epidemiology and pathophysiology . Clinical & experimental ophthalmology . 2013 Mar;41(2):201-14. Desai UR, Alhalel AA, Campen TJ, Schiffman RM, Edwards P A, Jacobsen GR. Central serous chorioretinopathy in African Americans. Journal of the National Medical Association. 2003 Jul;95(7):596. Ahlers C, Geitzenauer W , Stock G, Golbaz I, Schmidt-Erfurth U, Prünte C. Alterations of intraretinal layers in acute central serous chorioretinopathy . Acta ophthalmologica. 2009 Aug;87(5):511-6. Lin J, Chen R W . Central serous chorioretinopathy . InManual of Retinal Diseases 2016 (pp. 421-426). Springer, Cham. Lafaut B A, Leys AM, Snyers B, Rasquin F , De Laey JJ. Polypoidal choroidal vasculopathy in Caucasians. Graefe’ s archi ve for clinical and e xperimental ophthalmology . 2000 Sep 1;238(9):752-9. Iwama D, Tsujikaw a A, Sasahara M, Hirami Y , T amura H, Y oshimura N. Polypoidal choroidal vasculopathy with drusen. Japanese journal of ophthalmology . 2008 Apr 1;52(2):116-21. 9 Schatz H, Madeira D, Johnson RN, McDonald HR. Central Serous Chonoretinopathy Occurring in P atients 60 Y ears of Age and Older . Ophthalmology . 1992 Jan 1;99(1):63-7. Chumbley LC, Frank RN. Central serous retinopathy and pregnancy . American journal of ophthalmology . 1974 Feb 1;77(2):158-60. Maruko I, Iida T , Saito M, Nagayama D, Saito K. Clinical characteristics of exudativ e age-related macular degeneration in Japanese patients. American journal of ophthalmology . 2007 Jul 1;144(1):15-22. V inding T . Age-related macular degeneration. Macular changes, pre v alence and sex ratio: An epidemiological study of 1000 aged individuals. Acta ophthalmologica. 1989 Dec;67(6):609-16. V arma R, Fraser-Bell S, T an S, Klein R, Azen SP , Los Angeles Latino Eye Study Group. Prev alence of age-related macular degeneration in Latinos: the Los Angeles Latino eye study . Ophthalmology . 2004 Jul 1;111(7):1288-97. Rudnicka AR, Jarrar Z, W ormald R, Cook DG, Fletcher A, Owen CG. Age and gender variations in age-related macular degeneration pre valence in populations of European ancestry: a meta-analysis. Ophthalmology . 2012 Mar 1;119(3):571-80. Klein R, Klein BE, Knudtson MD, W ong TY , Cotch MF , Liu K, Burke G, Saad MF , Jacobs Jr DR. Pre valence of age-related macular degeneration in 4 racial/ethnic groups in the multi-ethnic study of atherosclerosis. Ophthalmology . 2006 Mar 1;113(3):373-80. Byeon SH, Lee SC, Oh HS, Kim SS, K oh HJ, Kw on O W . Incidence and clinical patterns of polypoidal choroidal vasculopath y in K orean patients. Japanese journal of ophthalmology . 2008 Feb 1;52(1):57-62. Y annuzzi LA, W ong D W , Sforzolini BS, Goldbaum M, T ang KC, Spaide RF , Freund KB, Slakter JS, Guyer DR, Sorenson J A, Fisher Y . Polypoidal choroidal vasculopathy and neov ascularized age-related macular degeneration. Archi ves of Ophthalmology . 1999 Nov 1;117(11):1503-10. Roberts P , Baumann B, Lammer J, Gerendas B, Kroisamer J, Bühl W , Pircher M, Hitzenber ger CK, Schmidt- Erfurth U, Sacu S. Retinal pigment epithelial features in central serous chorioretinopathy identified by polarization-sensitiv e optical coherence tomography . In v estigati ve ophthalmology & visual science. 2016 Apr 1;57(4):1595-603. Kitzmann AS, Pulido JS, Diehl NN, Hodge DO, Burke JP . The incidence of central serous chorioretinopathy in Olmsted County , Minnesota, 1980–2002. Ophthalmology . 2008 Jan 1;115(1):169-73. Kingma DP , W elling M. Auto-encoding v ariational bayes. arXiv preprint arXi v:1312.6114. 2013 Dec 20. Coates, A., Ng, A., and Lee, H. (2011). An analysis of single-layer netw orks in unsupervised feature learning. In Pr oceedings of the fourteenth international confer ence on artificial intelligence and statistics , pages 215–223. Coates, A. and Ng, A. Y . (2012). Learning feature representations with k-means. In Neural networks: T ric ks of the trade , pages 561–580. Springer . Goodfellow , I., Pouget-Abadie, J., Mirza, M., Xu, B., W arde-Farley , D., Ozair, S., Courville, A., and Bengio, Y . (2014). Generativ e adversarial nets. In Advances in neural information pr ocessing systems , pages 2672–2680. Hinton, G. E., Osindero, S., and T eh, Y .-W . (2006). A fast learning algorithm for deep belief nets. Neur al computation , 18(7):1527–1554. Hinton, G. E. and Salakhutdinov , R. R. (2006). Reducing the dimensionality of data with neural networks. science , 313(5786):504–507. Jolliffe, I. (2011). Principal component analysis . Springer . Le, Q. V ., Ranzato, M., Monga, R., Devin, M., Chen, K., Corrado, G. S., Dean, J., and Ng, A. Y . (2011). Building high-lev el features using large scale unsupervised learning. arXiv preprint . Lee, H., Grosse, R., Ranganath, R., and Ng, A. Y . (2009). Conv olutional deep belief networks for scalable unsupervised learning of hierarchical representations. In Pr oceedings of the 26th annual international confer ence on machine learning , pages 609–616. A CM. MacQueen, J. et al. (1967). Some methods for classification and analysis of multiv ariate observations. In Pr oceedings of the fifth Berkele y symposium on mathematical statistics and pr obability , volume 1, pages 281–297. Oakland, CA, USA. 10 Mirza, M. and Osindero, S. (2014). Conditional generativ e adversarial nets. arXiv pr eprint arXiv:1411.1784 . Ngiam, J., Khosla, A., Kim, M., Nam, J., Lee, H., and Ng, A. Y . (2011). Multimodal deep learning. In Pr oceedings of the 28th international confer ence on machine learning (ICML-11) , pages 689–696. Radford, A., Metz, L., and Chintala, S. (2015). Unsupervised representation learning with deep con v olutional generativ e adversarial netw orks. arXiv pr eprint arXiv:1511.06434 . Schmidhuber , J. (1992). Learning factorial codes by predictability minimization. Neural Computation , 4(6):863– 879. V incent, P ., Larochelle, H., Lajoie, I., Bengio, Y ., and Manzagol, P .-A. (2010). Stacked denoising autoencoders: Learning useful representations in a deep network with a local denoising criterion. Journal of machine learning r esear ch , 11(Dec):3371–3408. W agstaff, K., Cardie, C., Rogers, S., Schrödl, S., et al. (2001). Constrained k-means clustering with background knowledge. In Icml , volume 1, pages 577–584. W ay GP , Greene CS. Extracting a biologically relev ant latent space from cancer transcriptomes with variational autoencoders. BioRxiv . 2017 Jan 1:174474. Rampasek L, Hidru D, Smirnov P , Haibe-Kains B, Goldenber g A. Dr . V AE: Drug response variational autoen- coder . arXi v preprint arXi v:1706.08203. 2017 Jun 26. Cohen I, David EO, Netanyahu NS, Liscovitch N, Chechik G. Deepbrain: Functional representation of neu- ral in-situ hybridization images for gene ontology classification using deep conv olutional autoencoders. InInternational Conference on Artificial Neural Networks 2017 Sep 11 (pp. 287-296). Springer , Cham. 11
Original Paper
Loading high-quality paper...
Comments & Academic Discussion
Loading comments...
Leave a Comment