Automated Computer Evaluation of Acute Ischemic Stroke and Large Vessel Occlusion
Large vessel occlusion (LVO) plays an important role in the diagnosis of acute ischemic stroke. Identifying LVO of patients in the early stage on admission would significantly lower the probabilities of suffering from severe effects due to stroke or even save their lives. In this paper, we utilized both structural and imaging data from all recorded acute ischemic stroke patients in Hong Kong. Total 300 patients (200 training and 100 testing) are used in this study. We established three hierarchical models based on demographic data, clinical data and features obtained from computerized tomography (CT) scans. The first two stages of modeling are merely based on demographic and clinical data. Besides, the third model utilized extra CT imaging features obtained from deep learning model. The optimal cutoff is determined at the maximal Youden index based on 10-fold cross-validation. With both clinical and imaging features, the Level-3 model achieved the best performance on testing data. The sensitivity, specificity, Youden index, accuracy and area under the curve (AUC) are 0.930, 0.684, 0.614, 0.790 and 0.850 respectively.
💡 Research Summary
This paper presents the development and evaluation of a hierarchical machine learning model designed for the automated early prediction of Large Vessel Occlusion (LVO) in patients suspected of Acute Ischemic Stroke (AIS). The primary objective is to create a tool that can assist in rapid triage and diagnosis, which is critical for timely intervention with treatments like endovascular thrombectomy (EVT), thereby improving patient outcomes.
The study utilized a dataset of 300 AIS patients from Hong Kong’s territory-wide healthcare records, split into 200 for training and 100 for testing. The data encompassed three tiers: basic demographic information (age, gender), structured clinical data (medical history, vital signs like blood pressure, Glasgow Coma Scale scores), and non-contrast brain Computed Tomography (CT) scans performed within 24 hours of admission. The presence of LVO, the target variable, was independently verified by two cerebrovascular specialists.
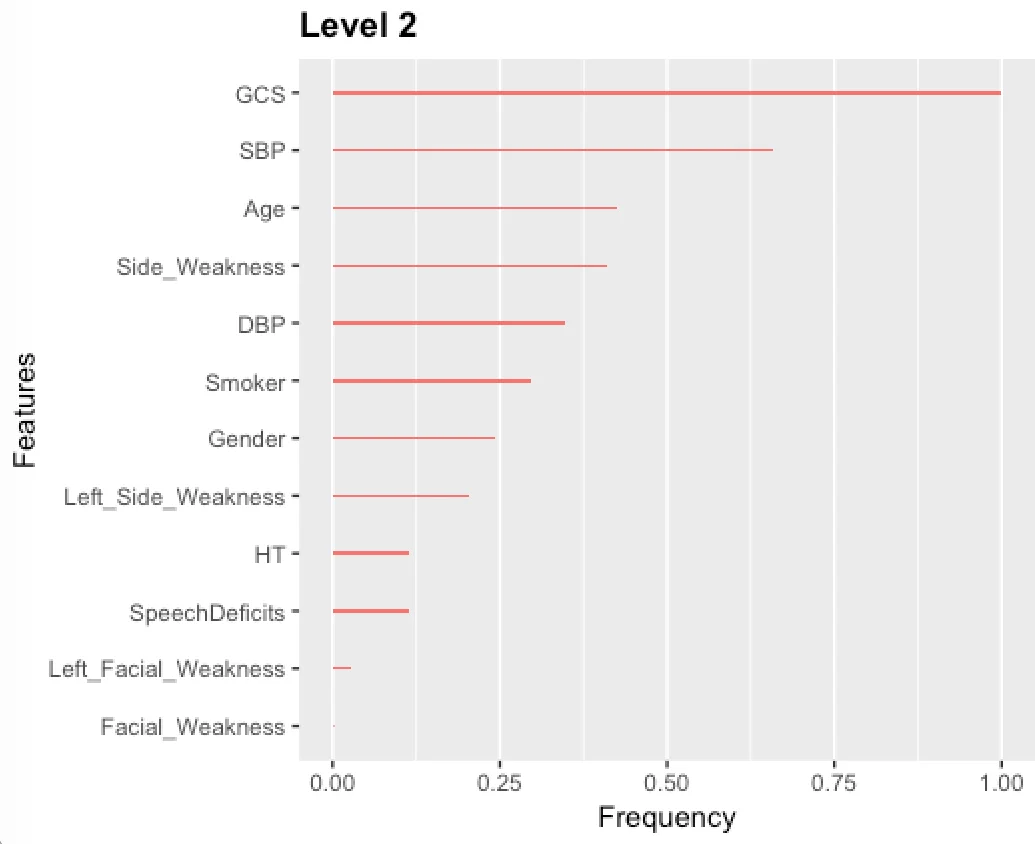
The methodological core is a three-level hierarchical modeling framework. Level-1 uses only easily obtainable demographic and basic symptom data. Level-2 incorporates all available structured clinical data. Level-3 further integrates imaging features extracted from the CT scans using a deep learning model. For image analysis, the researchers employed a preprocessing pipeline involving skull-stripping, registration, and thresholding, followed by a U-Net-like Fully Convolutional Network (FCN) to segment the hyperdense Middle Cerebral Artery (MCA) dot sign—a key radiological marker for LVO. High-level features from this network were extracted, and the top 10 most statistically significant features were selected via a two-sample t-test for inclusion in the Level-3 model. The eXtreme Gradient Boosting (XGBoost) classifier was chosen for all levels due to its robustness in handling missing values commonly found in clinical data, eliminating the need for separate imputation.
Model performance was evaluated using 10-fold cross-validation, with the optimal classification cutoff determined by maximizing the Youden Index, which balances sensitivity and specificity. Results on the independent test set showed progressive improvement across levels. The Level-1 model achieved an AUC of 0.647. The Level-2 model, enriched with clinical data, showed substantial gains, reaching an AUC of 0.809, a sensitivity of 93.0%, and a specificity of 64.9%. The final Level-3 model, which included imaging features, attained the best performance with an AUC of 0.850, a sensitivity of 93.0%, and a specificity of 68.4%.
The discussion highlights several key insights. The significant jump from Level-1 to Level-2 underscores the critical value of comprehensive clinical data in stroke assessment. The more modest improvement from Level-2 to Level-3 suggests that while imaging features add value, their impact in this study was limited. The authors attribute this partly to the deep learning model’s inability to correct false-positive cases that did not exhibit the MCA dot sign, and partly to the relatively small number of images with confirmed dot signs available for training. The choice of XGBoost is praised for its practical utility in real-world settings with incomplete data.
In conclusion, this research demonstrates the feasibility and promise of an automated, hierarchical AI model that combines demographic, clinical, and imaging data for the early prediction of LVO in stroke patients. While further validation with larger, multi-center datasets is needed, the model presents a potentially powerful decision-support tool to accelerate diagnosis and triage in emergency care settings, ultimately aiming to shorten the time to definitive treatment.
Comments & Academic Discussion
Loading comments...
Leave a Comment