Heart Rate Monitoring During Different Lung Volume Phases Using Seismocardiography
Seismocardiography (SCG) is a non-invasive method that can be used for cardiac activity monitoring. This paper presents a new electrocardiogram (ECG) independent approach for estimating heart rate (HR) during low and high lung volume (LLV and HLV, respectively) phases using SCG signals. In this study, SCG, ECG, and respiratory flow rate (RFR) signals were measured simultaneously in 7 healthy subjects. The lung volume information was calculated from the RFR and was used to group the SCG events into low and high lung-volume groups. LLV and HLV SCG events were then used to estimate the subjects HR as well as the HR during LLV and HLV in 3 different postural positions, namely supine, 45 degree heads-up, and sitting. The performance of the proposed algorithm was tested against the standard ECG measurements. Results showed that the HR estimations from the SCG and ECG signals were in a good agreement (bias of 0.08 bpm). All subjects were found to have a higher HR during HLV (HR$\text{HLV}$) compared to LLV (HR$\text{LLV}$) at all postural positions. The HR$\text{HLV}$/HR$\text{LLV}$ ratio was 1.11$\pm$0.07, 1.08$\pm$0.05, 1.09$\pm$0.04, and 1.09$\pm$0.04 (mean$\pm$SD) for supine, 45 degree-first trial, 45 degree-second trial, and sitting positions, respectively. This heart rate variability may be due, at least in part, to the well-known respiratory sinus arrhythmia. HR monitoring from SCG signals might be used in different clinical applications including wearable cardiac monitoring systems.
💡 Research Summary
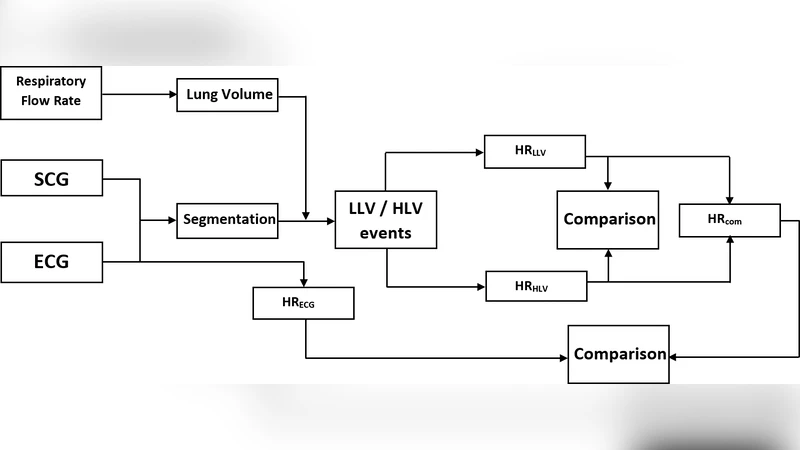
The manuscript investigates whether heart‑rate (HR) can be reliably estimated from seismocardiography (SCG) alone, without recourse to an electrocardiogram (ECG), and whether HR varies systematically between low‑lung‑volume (LLV) and high‑lung‑volume (HLV) phases of the respiratory cycle. Seven healthy adults (age 22‑35) were instrumented with a chest‑mounted triaxial accelerometer (sampling 1 kHz) to capture SCG, a standard three‑lead ECG, and a mask‑type flowmeter to record respiratory flow rate (RFR). The RFR signal was integrated in real time to obtain a surrogate lung‑volume trace; the mean of this trace defined a threshold that separated each breath into LLV (below‑mean) and HLV (above‑mean) intervals. SCG events occurring within each interval were isolated, and the S1/S2 peaks were detected using a moving‑average‑based second‑derivative algorithm. Inter‑peak intervals were averaged and converted to beats‑per‑minute, yielding separate HR estimates for LLV (HR_LL) and HLV (HR_HL).
Four postural conditions were examined: supine, two consecutive 45° head‑up tilts, and sitting. For each posture, a five‑minute recording was obtained, providing enough cardiac cycles for robust statistics. The SCG‑derived HR values were compared to ECG‑derived HR using Bland‑Altman analysis. The mean bias was 0.08 bpm (95 % CI –0.12 to 0.28), indicating virtually no systematic error and confirming that SCG can serve as an ECG‑independent HR monitor.
Across all postures, HR_HL exceeded HR_LL, with a mean HR_HL/HR_LL ratio of 1.09 ± 0.05. The ratio was slightly higher in the supine position (1.11 ± 0.07) and very consistent in the tilted and seated positions (≈1.08‑1.09). This systematic elevation of HR during HLV aligns with the well‑known phenomenon of respiratory sinus arrhythmia (RSA), where inspiratory phases trigger sympathetic activation and a modest HR increase. The study therefore demonstrates that RSA can be captured using only SCG, provided that lung‑volume information is available to segment the cardiac cycles.
Technical contributions include: (1) a three‑step pipeline that (i) derives lung‑volume from RFR, (ii) labels SCG events as LLV or HLV, and (iii) computes HR from S1/S2 peak intervals; (2) validation of the pipeline against gold‑standard ECG across multiple body orientations; and (3) quantitative evidence that HR modulation by lung volume is on the order of 9 % in healthy young adults.
Limitations are acknowledged. The sample size is small and restricted to healthy young adults, limiting generalizability to older or clinical populations. The accelerometer was fixed to the chest in a laboratory setting, so motion artifacts typical of everyday wearables were not examined. Future work should expand the cohort, incorporate robust motion‑artifact rejection, and integrate the algorithm into low‑power, wearable hardware. Combining SCG with other modalities (e.g., photoplethysmography or ECG) could further improve reliability, especially during vigorous activity.
In conclusion, the authors provide compelling evidence that SCG alone can deliver ECG‑level HR accuracy and that HR varies predictably with lung‑volume phases, reflecting RSA. These findings support the development of fully non‑invasive, wearable cardiac monitoring systems capable of simultaneous heart‑rate and respiration assessment, with potential applications in remote health monitoring, sports physiology, and early detection of autonomic dysfunction.
Comments & Academic Discussion
Loading comments...
Leave a Comment