An Adaptive Feature Extraction Algorithm for Classification of Seismocardiographic Signals
This paper proposes a novel adaptive feature extraction algorithm for seismocardiographic (SCG) signals. The proposed algorithm divides the SCG signal into a number of bins, where the length of each bin is determined based on the signal change within that bin. For example, when the signal variation is steeper, the bins are shorter and vice versa. The proposed algorithm was used to extract features of the SCG signals recorded from 7 healthy individuals (Age: 29.4$\pm$4.5 years) during different lung volume phases. The output of the feature extraction algorithm was fed into a support vector machines classifier to classify SCG events into two classes of high and low lung volume (HLV and LLV). The classification results were compared with currently available non-adaptive feature extraction methods for different number of bins. Results showed that the proposed algorithm led to a classification accuracy of ~90%. The proposed algorithm outperformed the non-adaptive algorithm, especially as the number of bins was reduced. For example, for 16 bins, F1 score for the adaptive and non-adaptive methods were 0.91$\pm$0.05 and 0.63$\pm$0.08, respectively.
💡 Research Summary
The paper introduces an adaptive feature‑extraction algorithm tailored for seismocardiographic (SCG) signals, which are mechanical vibrations generated by cardiac activity and recorded at the chest surface. Traditional SCG analysis often relies on fixed‑length segmentation (bins) to compute simple statistical descriptors such as mean, variance, or spectral power. Because SCG waveforms contain rapid, high‑amplitude events (e.g., the S1 and S2 heart sounds) interspersed with relatively flat portions, a uniform binning strategy inevitably discards important temporal information, especially when the number of bins is limited for computational or storage reasons.
The proposed method dynamically adjusts bin lengths according to the magnitude of signal change within a segment. After low‑pass filtering (≈20–50 Hz) to suppress high‑frequency noise, the algorithm computes the absolute first‑difference of the signal and accumulates it. When the cumulative change exceeds a pre‑defined threshold, a new bin is started; otherwise, the current bin continues to grow. This threshold is empirically tuned so that the total number of bins can be constrained (e.g., 16, 32, 64) while still allocating short bins to steep portions of the waveform and longer bins to slowly varying sections.
For each adaptive bin, a feature vector is constructed comprising: (1) time‑domain statistics (mean, max, min, standard deviation), and (2) frequency‑domain descriptors obtained from a short‑time Fourier transform (dominant frequencies and power in the 1–10 Hz band). The resulting feature matrix has a dimensionality equal to the number of bins multiplied by the number of descriptors per bin.
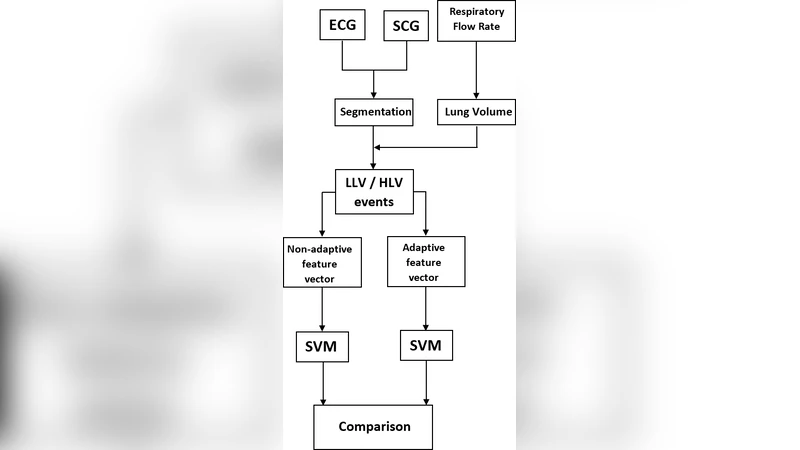
The authors collected SCG recordings from seven healthy volunteers (mean age 29.4 ± 4.5 years) under two controlled lung‑volume conditions: low lung volume (LLV) and high lung volume (HLV). Each condition lasted 30 seconds, providing a clear physiological contrast because lung inflation shifts the heart’s position and alters the transmission path of mechanical vibrations. The adaptive features were fed into a linear‑kernel support vector machine (SVM) classifier. Model hyper‑parameters (the penalty parameter C) were optimized via five‑fold cross‑validation, and performance metrics (accuracy, precision, recall, F1‑score) were reported for each bin count.
A non‑adaptive baseline was implemented by dividing each SCG record into equally sized bins and extracting the same set of descriptors. When the bin count was high (64 bins), both methods achieved comparable accuracies (~92%). However, as the number of bins decreased, the fixed‑bin approach suffered a steep performance drop: with 16 bins, accuracy fell to ~68% and the F1‑score averaged 0.63 ± 0.08. In contrast, the adaptive method retained high discriminative power, delivering an average accuracy of ~90% and an F1‑score of 0.91 ± 0.05 for the same 16‑bin configuration. The superiority of the adaptive scheme is attributed to its ability to preserve the timing and morphology of critical SCG events, which are highly informative for distinguishing between LLV and HLV states.
The study’s limitations include a small, homogenous sample (young, healthy adults), which restricts the generalizability of the findings to older populations or patients with cardiovascular or pulmonary pathology. Moreover, the classification pipeline relies on a conventional SVM; modern deep‑learning architectures such as convolutional neural networks (CNNs) or long short‑term memory (LSTM) networks, which can learn hierarchical temporal features directly from raw waveforms, were not evaluated. Real‑time deployment considerations (e.g., computational load on wearable hardware) and robustness to motion artifacts also remain open questions.
Future work suggested by the authors encompasses: (i) expanding the dataset to include diverse age groups, genders, and clinical conditions; (ii) integrating the adaptive binning concept with end‑to‑end neural models to assess whether the adaptive segmentation can serve as a preprocessing step that improves deep‑learning performance; (iii) exploring multi‑class classification that includes intermediate lung‑volume levels; and (iv) implementing the algorithm on low‑power embedded platforms for continuous, ambulatory monitoring.
In summary, the paper demonstrates that a signal‑change‑driven, adaptive binning strategy can extract compact yet highly informative features from SCG recordings, outperforming traditional fixed‑bin methods especially when the feature budget is limited. This approach holds promise for enhancing non‑invasive cardiac‑respiratory monitoring systems, potentially enabling real‑time assessment of lung volume and cardiac mechanics in both clinical and wearable health‑tech applications.
Comments & Academic Discussion
Loading comments...
Leave a Comment