Does the Position of Surgical Service Providers in Intra-Operative Networks Matter? Analyzing the Impact of Influencing Factors on Patients Outcome
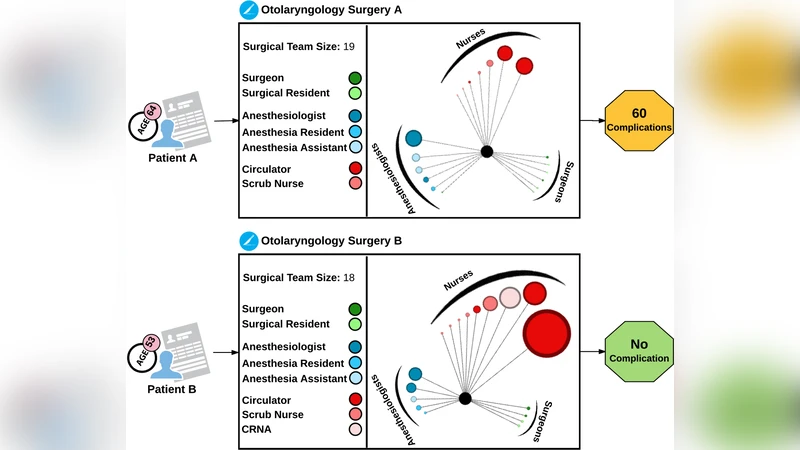
We analyzed the relation between surgical service providers’ network structure and surgical team size with patient outcome during the operation. We did correlation analysis to evaluate the associations among the network structure measures in the intra-operative networks of surgical service providers. We focused on intra-operative networks of surgical service providers, in a quaternary-care academic medical center, using retrospective Electronic Medical Record (EMR) data. We used de-identified intra-operative data for adult patients who received nonambulatory/nonobstetric surgery in a main operating room at Shands at the University of Florida between June 1, 2011 and November 1, 2014. The intra-operative dataset contained 30,211 unique surgical cases. To perform the analysis, we created the networks of surgical service providers and calculated several network structure measures at both team and individual levels. We considered number of patients’ complications as the target variable and assessed its interrelations with the calculated network measures along with other influencing factors (e.g. surgical team size, type of surgery). Our results confirm the significant role of interactions among surgical providers on patient outcome. In addition, we observed that highly central providers at the global network level are more likely to be associated with a lower number of surgical complications, while locally important providers might be associated with higher number of complications. We also found a positive relation between age of patients and number of complications.
💡 Research Summary
This study investigates how the structural position of surgical service providers within intra‑operative collaboration networks relates to postoperative complication rates. Using de‑identified electronic medical record data from the University of Florida’s Shands Hospital, the authors assembled a retrospective cohort of 30,211 adult, non‑ambulatory, non‑obstetric surgeries performed between June 1, 2011 and November 1, 2014. To capture temporal dynamics, the four‑year span was divided into four consecutive one‑year segments; for each segment a bipartite (two‑mode) network was built linking providers to the cases they participated in, then projected onto a one‑mode provider‑only graph where edges represent shared cases.
For every provider in each yearly network, five classic graph‑theoretic measures were computed: degree centrality, betweenness centrality, closeness centrality, clustering coefficient, and eigenvector centrality. Because of multicollinearity, degree and clustering were excluded from the regression models, leaving betweenness, closeness, and eigenvector centralities as the primary network predictors. In addition to these network variables, patient‑level covariates (age, gender, race, ethnicity, marital status, body‑mass index, Charlson comorbidity index, length of stay), surgical variables (team size, service type, principal diagnosis and procedure), and temporal indicators were merged to create a comprehensive “Surgical Network Data” set.
The outcome variable was the count of postoperative complications, derived from ICD‑9‑CM codes (996‑999) identified across up to 50 diagnosis fields per admission. Complications were treated as a performance proxy for the surgical team, acknowledging that not all complications imply procedural error.
Statistical analysis comprised pairwise correlation among all network metrics, followed by generalized linear modeling (Poisson or negative‑binomial, depending on dispersion) to assess the independent contribution of each predictor to complication count. The key findings are:
-
Global network centrality matters – Higher betweenness and eigenvector centralities (reflecting “brokers” and “leaders” who connect disparate groups or are linked to other well‑connected providers) were significantly associated with fewer complications. This suggests that providers occupying strategic bridging positions facilitate efficient information flow, rapid decision‑making, and perhaps better coordination during surgery.
-
Local density can be detrimental – Higher closeness centrality, which indicates that a provider is on average closer to many others within the same sub‑network, correlated with more complications. The authors interpret this as a possible “over‑clustering” effect where tightly knit sub‑groups may limit exposure to diverse expertise, amplify groupthink, or accelerate error propagation.
-
Team size shows a non‑linear relationship – Larger teams were generally linked to higher complication counts, but the effect plateaued beyond roughly six to eight members, echoing prior work on the trade‑off between resource availability and communication overhead.
-
Surgical volume and team consistency improve outcomes – Higher annual case volume and repeated use of the same team composition (team consistency) were associated with reduced complications, supporting the notion that experience and stable teamwork enhance performance.
-
Patient age is the strongest clinical predictor – Each additional year of age increased the expected complication count by about 2 %, even after adjusting for comorbidities, BMI, and other covariates. This aligns with established geriatric risk profiles.
The study acknowledges several limitations: its observational design precludes causal inference; the yearly segmentation may miss finer‑grained network evolution; provider roles (surgeon, anesthesiologist, circulating nurse, trainee) were not differentiated in the centrality calculations, potentially conflating distinct functional contributions; and the exclusion of two network metrics due to multicollinearity reduced the dimensionality of the analysis.
Despite these constraints, the work demonstrates the feasibility and value of applying social network analysis to intra‑operative settings. It suggests that hospital administrators could monitor provider‑level network metrics in real time, deliberately position high‑betweenness individuals in critical cases, and avoid overly dense sub‑teams that may hinder performance. Future research directions include role‑specific centrality analyses, dynamic (e.g., monthly) network reconstruction, incorporation of surgical complexity scores, and experimental designs (e.g., randomized team assignments) to test causality.
In conclusion, the structural position of surgical providers within intra‑operative collaboration networks is significantly linked to postoperative complication rates. Global centrality appears protective, while excessive local closeness may increase risk. These insights add a network‑centric dimension to existing quality‑improvement strategies, highlighting the potential of network‑guided team composition to enhance patient safety.
Comments & Academic Discussion
Loading comments...
Leave a Comment