A rule-based system proposal to aid in the evaluation and decision-making in external beam radiation treatment planning
As part of a plan launched by the Ministry of Health of Brazil to increase the availability of linear accelerators for radiotherapy treatment for the whole country, for which Varian Medical Systems company has won the bidding, a technical cooperation agreement was signed inviting Brazilian Scientific and Technological Institutions to participate in a technology transfer program. As a result, jointly, the Eldorado Research Institute and the Center for Biomedical Engineering of the University of Campinas presents in this work, the concepts behind of a proposed rule engine to aid in the evaluation and decision-making in radiotherapy treatment planning. Normally, the determination of the radiation dose for a given patient is a complex and intensive procedure, which requires a lot of domain knowledge and subjective experience from the oncologists’ team. In order to help them in this complex task, and additionally, provide an auxiliary tool for less experienced oncologists, it is presented a project conception of a software system that will make use of a hybrid data-oriented approach. The proposed rule engine will apply both inference mechanism and expression evaluation to verify and accredit the quality of an external beam radiation treatment plan by considering, at first, the 3D-conformal radiotherapy (3DCRT) technique.
💡 Research Summary
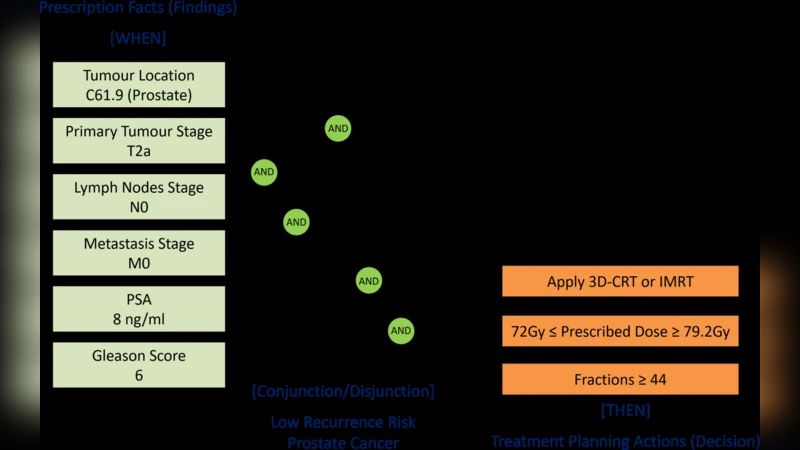
The paper presents a proposal for a rule‑based decision‑support system aimed at improving the evaluation and planning of external beam radiotherapy (EBRT), specifically focusing on the 3‑dimensional conformal radiotherapy (3D‑CRT) technique. The work originates from a Brazilian Ministry of Health initiative to expand linear accelerator availability across the country, with Varian Medical Systems supplying the equipment. In response, the Eldorado Research Institute and the Center for Biomedical Engineering at the University of Campinas (UNICAMP) collaborated to design a software prototype that combines two complementary engines: a logical inference engine that encodes clinical guidelines, institutional policies, and expert knowledge as IF‑THEN rules (using a medical‑oriented syntax such as Arden), and an expression‑evaluation engine that computes quantitative dosimetric metrics (e.g., DVH parameters, conformity index, homogeneity index) and compares them against rule‑defined thresholds.
The architecture is organized into three layers. The data acquisition layer imports DICOM‑RT objects (structures, dose matrices, beam configurations), normalizes them, and stores them in an internal representation. The rule‑engine layer processes the normalized data, firing applicable rules and generating a set of compliance scores and violation reports. The visualization layer provides a web‑based dashboard that displays rule outcomes, numeric quality indicators, and suggested corrective actions for the planner. By applying rules at each planning stage—contouring, beam placement, dose calculation, and final verification—the system seeks to increase intra‑planner and inter‑planner consistency, embed local cultural and policy nuances, and create both qualitative and quantitative plan‑quality metrics.
Key objectives include: (1) reducing variability among planners; (2) allowing each radiotherapy center to inject its specific context into the rule set; (3) identifying prognostic quality features that can guide plan improvement; and (4) enabling the development of composite metrics that combine expert opinion with objective dosimetric data. The authors illustrate the workflow with a detailed description of the conventional 3D‑CRT forward‑planning process, highlighting the iterative nature of beam adjustment and the potential for the rule engine to shorten the number of iterations by providing real‑time feedback.
Strengths of the proposal are its clear alignment with clinical practice, the use of a hybrid approach that preserves rule readability while delivering fast numerical evaluation, and the focus on supporting less‑experienced oncologists. The system also promises to facilitate training and standardization across Brazil’s public health network (SUS). However, several limitations are acknowledged. The current design is limited to 3D‑CRT and does not yet address inverse‑planning modalities such as IMRT or VMAT, which involve more complex optimization that a pure rule‑based engine cannot solve alone. Maintaining and updating the rule base to reflect evolving guidelines will require dedicated governance. Moreover, the paper lacks a large‑scale clinical validation; without extensive testing on diverse patient cohorts, the sensitivity, specificity, and impact on clinical outcomes remain uncertain. Integration with existing treatment planning systems (TPS) depends on robust DICOM‑RT handling and version control, and regulatory approval (e.g., ANVISA, FDA) will add further development overhead.
In conclusion, the work demonstrates the feasibility of embedding expert knowledge and institutional policies into a rule‑based framework for EBRT plan quality assessment. While promising as a decision‑support and educational tool, future work must extend the rule set to advanced planning techniques, implement automated rule‑maintenance pipelines, and conduct multi‑institutional clinical trials to substantiate its efficacy and safety. Successful maturation could enhance treatment consistency, reduce planning time, and ultimately improve patient outcomes within Brazil’s public oncology services and beyond.
Comments & Academic Discussion
Loading comments...
Leave a Comment