Making effective use of healthcare data using data-to-text technology
Healthcare organizations are in a continuous effort to improve health outcomes, reduce costs and enhance patient experience of care. Data is essential to measure and help achieving these improvements in healthcare delivery. Consequently, a data influx from various clinical, financial and operational sources is now overtaking healthcare organizations and their patients. The effective use of this data, however, is a major challenge. Clearly, text is an important medium to make data accessible. Financial reports are produced to assess healthcare organizations on some key performance indicators to steer their healthcare delivery. Similarly, at a clinical level, data on patient status is conveyed by means of textual descriptions to facilitate patient review, shift handover and care transitions. Likewise, patients are informed about data on their health status and treatments via text, in the form of reports or via ehealth platforms by their doctors. Unfortunately, such text is the outcome of a highly labour-intensive process if it is done by healthcare professionals. It is also prone to incompleteness, subjectivity and hard to scale up to different domains, wider audiences and varying communication purposes. Data-to-text is a recent breakthrough technology in artificial intelligence which automatically generates natural language in the form of text or speech from data. This chapter provides a survey of data-to-text technology, with a focus on how it can be deployed in a healthcare setting. It will (1) give an up-to-date synthesis of data-to-text approaches, (2) give a categorized overview of use cases in healthcare, (3) seek to make a strong case for evaluating and implementing data-to-text in a healthcare setting, and (4) highlight recent research challenges.
💡 Research Summary
The chapter provides a comprehensive survey of data‑to‑text (D2T) technology and its potential to transform the way healthcare organizations handle the ever‑growing influx of clinical, financial, and operational data. It begins by outlining the fundamental problem: while data are essential for measuring outcomes, reducing costs, and improving patient experience, converting these data into readable reports remains a labor‑intensive, error‑prone activity performed by clinicians and administrators. Textual reports are indispensable for decision‑making, hand‑overs, and patient communication, yet their manual creation limits scalability and consistency.
The authors introduce the canonical D2T pipeline, which consists of five sequential stages: (1) “What is known” – the representation of domain knowledge using standardized ontologies such as SNOMED‑CT and OBO Foundry; (2) “What can be said” – data analysis, abstraction, and interpretation, which may involve time‑series processing, statistical KPI calculation, or risk estimation; (3) “What to say” – content determination and text structuring, where the system decides which information‑bearing items to include and in what order, often employing Rhetorical Structure Theory (RST) to model causal, temporal, and contrastive relations; (4) “How to say it” – sentence aggregation, lexicalisation, and referring expression generation, which shape the linguistic form, choose appropriate terminology for the target audience, and reduce redundancy; and (5) “Actually saying it” – linguistic realisation, producing a well‑formed, coherent natural‑language output.
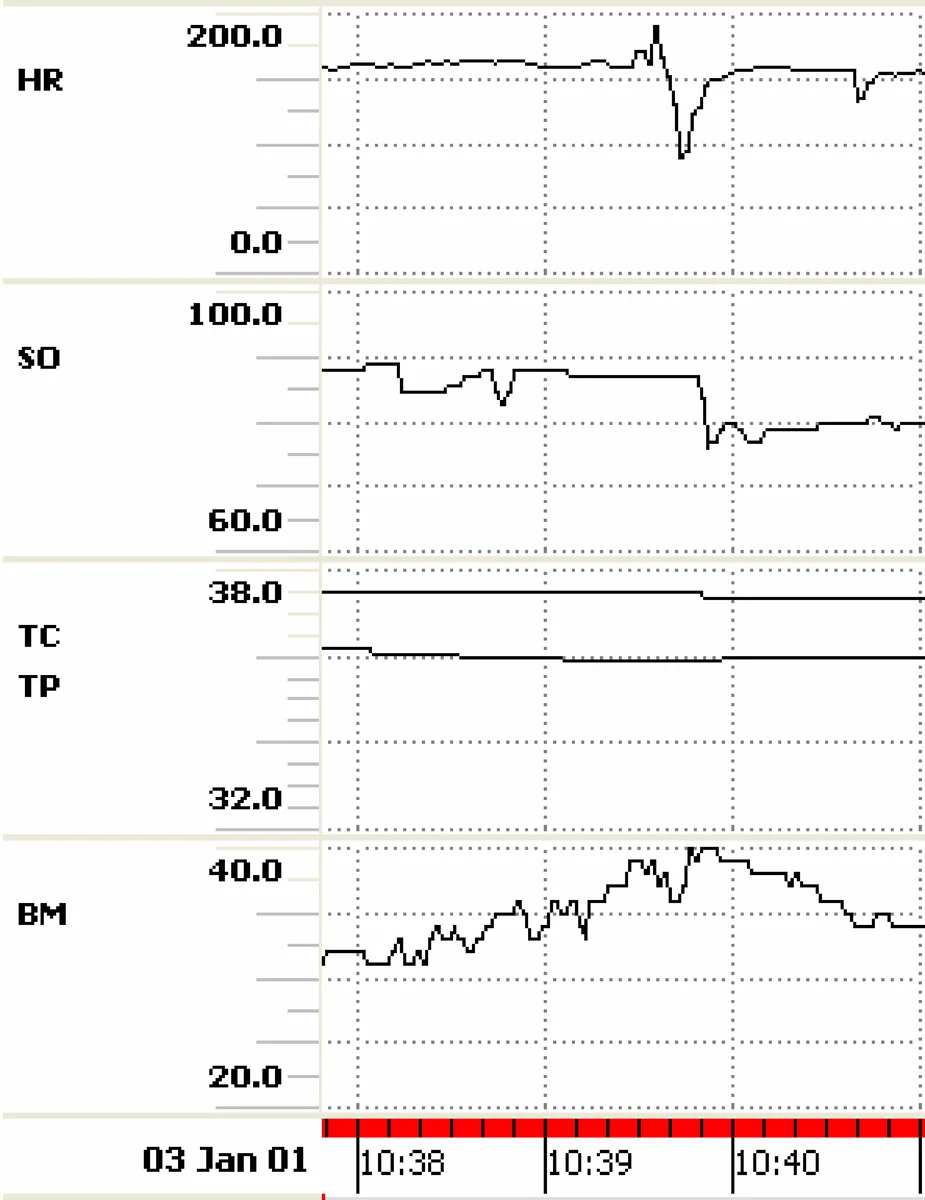
Through a detailed case study of the Babytalk BT‑45 system, the chapter illustrates each stage in practice. BT‑45 ingests 45 minutes of neonatal intensive care unit (NICU) sensor data (heart rate, oxygen saturation, blood pressure, temperature) and, using a custom NICU ontology and expert‑derived rules, identifies clinically relevant events such as bradycardia, desaturation, a blood‑pressure spike, and a morphine administration. Importance scores guide content selection, RST graphs encode that morphine may have caused downstream physiological changes, and aggregation rules merge cardiovascular events into a single sentence. The final output – a 23‑word summary – demonstrates how D2T can compress complex multimodal data into concise, actionable narrative.
The authors then categorize healthcare use cases into three broad domains: (a) financial reporting, where D2T automatically generates KPI‑driven executive summaries; (b) clinical documentation, including bedside monitoring summaries, radiology report generation, and shift‑hand‑over notes; and (c) patient‑facing communication, where personalized explanations of diagnoses, treatment plans, and self‑care instructions are produced in lay language. Each domain presents distinct requirements for input data types, audience tailoring, tone, and regulatory compliance.
Implementation considerations are discussed in depth. Evaluation must balance automatic metrics (BLEU, ROUGE, METEOR) with clinical effectiveness measures such as reduced chart‑review time, lower error rates, and improved patient understanding. System design must support audience‑specific style sheets, multilingual output, real‑time processing, and strict privacy/security standards (e.g., HIPAA). The chapter also highlights the tension between rule‑based, knowledge‑engineered approaches and data‑driven deep learning models, suggesting hybrid architectures that leverage the interpretability of rules with the adaptability of neural networks.
Finally, the chapter outlines open research challenges: (i) automated ontology evolution and maintenance; (ii) robust handling of noisy, incomplete, or biased data; (iii) scalable learning from large, heterogeneous clinical corpora; (iv) continuous user‑feedback loops for personalization and error correction; and (v) formal frameworks for ethical, legal, and regulatory validation of automatically generated medical text.
In conclusion, the authors make a strong case that data‑to‑text technology can alleviate the administrative burden on clinicians, ensure consistency and timeliness of medical narratives, and enhance patient engagement—all while supporting the broader goals of cost reduction, outcome improvement, and experience optimization in modern healthcare systems.
Comments & Academic Discussion
Loading comments...
Leave a Comment