Cardiac Arrhythmia Detection from ECG Combining Convolutional and Long Short-Term Memory Networks
Objectives: Atrial fibrillation (AF) is a common heart rhythm disorder associated with deadly and debilitating consequences including heart failure, stroke, poor mental health, reduced quality of life and death. Having an automatic system that diagnoses various types of cardiac arrhythmias would assist cardiologists to initiate appropriate preventive measures and to improve the analysis of cardiac disease. To this end, this paper introduces a new approach to detect and classify automatically cardiac arrhythmias in electrocardiograms (ECG) recordings. Methods: The proposed approach used a combination of Convolution Neural Networks (CNNs) and a sequence of Long Short-Term Memory (LSTM) units, with pooling, dropout and normalization techniques to improve their accuracy. The network predicted a classification at every 18th input sample and we selected the final prediction for classification. Results were cross-validated on the Physionet Challenge 2017 training dataset, which contains 8,528 single lead ECG recordings lasting from 9s to just over 60s. Results: Using the proposed structure and no explicit feature selection, 10-fold stratified cross-validation gave an overall F-measure of 0.83.10-0.015 on the held-out test data (mean-standard deviation over all folds) and 0.80 on the hidden dataset of the Challenge entry server.
💡 Research Summary
**
The paper addresses the clinically critical problem of automatically detecting and classifying cardiac arrhythmias, especially atrial fibrillation (AF), from single‑lead electrocardiogram (ECG) recordings. Traditional automated solutions rely heavily on handcrafted features such as R‑peak detection, heart‑rate variability metrics, and morphological descriptors, which are vulnerable to noise, variable recording lengths, and inter‑patient variability. To overcome these limitations, the authors propose an end‑to‑end deep learning framework that ingests raw ECG waveforms without any explicit preprocessing or feature engineering.
The architecture consists of two main components. First, a one‑dimensional convolutional neural network (CNN) extracts local temporal patterns (P‑waves, QRS complexes, T‑waves) from the raw signal. The CNN stack includes multiple convolutional layers with varying kernel sizes, interleaved with max‑pooling, batch‑normalization, and dropout layers. This design captures multi‑scale information and reduces overfitting while preserving sufficient temporal resolution across recordings that range from 9 seconds to over 60 seconds. Parallel convolutional branches further enrich the feature set by learning complementary receptive fields.
Second, the sequence of feature maps produced by the CNN is fed into a stacked Long Short‑Term Memory (LSTM) network. Two LSTM layers, each with 128 hidden units, model long‑range dependencies such as the temporal evolution of heart‑rate irregularities, the duration of abnormal episodes, and the context surrounding arrhythmic events. By combining CNN‑derived local descriptors with LSTM’s ability to capture global dynamics, the model can discriminate between normal rhythm, AF, other arrhythmias, and noisy recordings more robustly than either component alone.
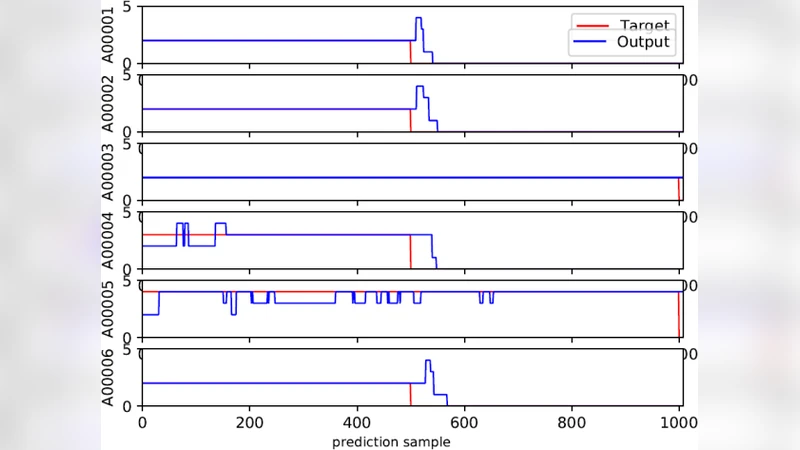
Training is performed on the PhysioNet 2017 Challenge dataset, which contains 8,528 single‑lead ECG recordings annotated into four classes. To mitigate class imbalance, the loss function is a weighted cross‑entropy where minority classes receive higher weights. Data augmentation strategies—random time‑shifts, additive Gaussian noise, and amplitude scaling—are applied on‑the‑fly to improve generalization. The network makes a prediction every 18 samples; the final classification for a recording is taken as the majority vote across all windows, a “sliding‑window” scheme that reduces computational load while preserving accuracy.
Evaluation uses stratified 10‑fold cross‑validation. The proposed CNN‑LSTM model achieves an overall F‑measure of 0.83 ± 0.015, outperforming baseline CNN‑only and LSTM‑only configurations reported in the literature. Notably, recall for the rare arrhythmia classes improves, indicating that the combined architecture successfully captures both short‑term morphological cues and long‑term rhythm patterns. On the hidden test set of the Challenge server, the model attains an F‑measure of 0.80, demonstrating its robustness in a blind evaluation scenario.
Key contributions of the work include: (1) eliminating the need for handcrafted ECG features, thereby simplifying the pipeline and reducing domain‑specific preprocessing; (2) demonstrating that a hybrid CNN‑LSTM architecture can synergistically exploit local waveform morphology and global temporal context; (3) introducing a computationally efficient sliding‑window inference strategy suitable for real‑time monitoring applications.
The study also acknowledges several limitations. It is confined to single‑lead ECG, whereas multi‑lead recordings could provide additional spatial information. The model operates as a black box, offering limited interpretability for clinicians; techniques such as attention mechanisms or saliency mapping could address this. Finally, the robustness of the system against real‑world artifacts (e.g., electrode detachment, motion noise) remains to be thoroughly validated.
Future research directions suggested by the authors involve extending the framework to multi‑lead inputs, integrating attention layers to highlight diagnostically relevant time points, applying model compression and quantization for deployment on wearable devices, and employing explainable‑AI methods (e.g., SHAP, Grad‑CAM) to increase clinical trust. By pursuing these avenues, the proposed approach has the potential to evolve from a research prototype into a reliable decision‑support tool that assists cardiologists in early arrhythmia detection and improves patient outcomes.
Comments & Academic Discussion
Loading comments...
Leave a Comment