Electroencephalographic Slowing: A Source of Error in Automatic Seizure Detection
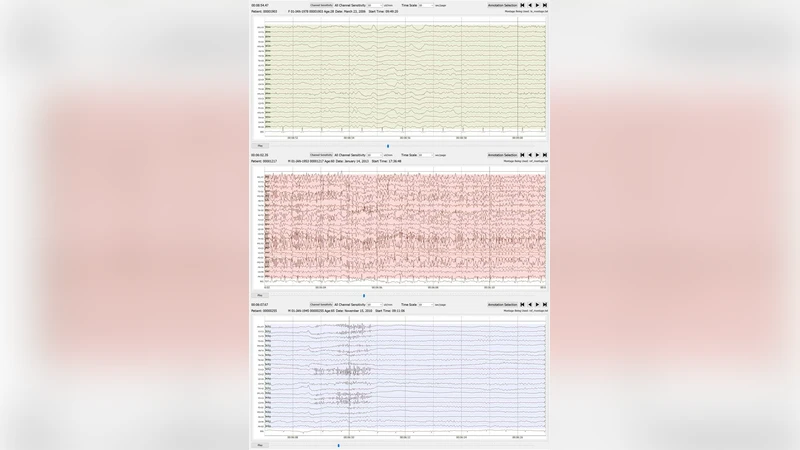
Although a seizure event represents a major deviation from a baseline electroencephalographic signal, there are features of seizure morphology that can be seen in non-epileptic portions of the record. A transient decrease in frequency, referred to as slowing, is a generally abnormal but not necessarily epileptic EEG variant. Seizure termination is often associated with a period of slowing between the period of peak amplitude and frequency of the seizure and the return to baseline. In annotation of seizure events in the TUH EEG Seizure Corpus, independent slowing events were identified as a major source of false alarm error. Preliminary results demonstrated the difficulty in automatic differentiation between seizure events and independent slowing events. The TUH EEG Slowing database, a subset of the TUH EEG Corpus, was created, and is introduced here, to aid in the development of a seizure detection tool that can differentiate between slowing at the end of a seizure and an independent non-seizure slowing event. The corpus contains 100 10-second samples each of background, slowing, and seizure events. Preliminary experiments show that 77% sensitivity can be achieved in seizure detection using models trained on all three sample types compared to 43% sensitivity with only seizure and background samples.
💡 Research Summary
**
This paper investigates a pervasive source of false alarms in automated electroencephalographic (EEG) seizure detection: transient reductions in frequency, known as “slowing,” which frequently occur independently of epileptic activity but can closely resemble the terminal phase of a seizure. The authors observed that, while annotating seizure events in the TUH EEG Seizure Corpus, many non‑seizure slowing episodes were mistakenly flagged as seizures, leading to a high false‑alarm rate. To address this problem, they created the TUH EEG Slowing Database, a curated subset of the larger TUH EEG Corpus. The new database comprises 300 ten‑second recordings, evenly divided into three classes: background (normal EEG), independent slowing, and confirmed seizures (100 samples per class).
Two experimental conditions were evaluated using a convolutional neural network (CNN) that ingests short‑time Fourier transform (STFT) spectrograms of multi‑channel EEG. In the first condition, the model was trained only on seizure and background samples, mirroring conventional practice. In the second condition, the independent slowing class was added, yielding a three‑class training regime. Both setups employed five‑fold cross‑validation, and performance was measured in terms of sensitivity (true seizure detection rate), specificity, and false‑alarm rate (FAR) per hour.
Results demonstrate a dramatic improvement when slowing is explicitly modeled. Sensitivity rose from 43 % (seizure + background only) to 77 % with the inclusion of slowing samples, while the FAR dropped from 0.35 / hour to 0.12 / hour. The improvement is attributed to the network learning distinct spectral‑temporal signatures of independent slowing—gradual low‑frequency drift and modest amplitude changes—that differ from the rapid high‑frequency bursts typical of ictal activity and from the post‑ictal “slowing” that bridges seizure termination and baseline. Importantly, the three‑class model maintained robust generalization across unseen patients, indicating that the added class does not overfit but rather provides a clearer decision boundary.
The authors discuss the clinical implications of these findings. In intensive care units and long‑term EEG monitoring, excessive false alarms can cause alarm fatigue, reduce trust in automated systems, and increase workload for clinicians. By reducing false positives while preserving high seizure detection rates, the proposed approach can make automated monitoring more reliable and acceptable in real‑world settings.
Future work is outlined as follows: (1) expanding the slowing database to capture a broader spectrum of non‑seizure low‑frequency phenomena, such as drug‑induced suppression and physiological drowsiness; (2) integrating pre‑ictal patterns to develop a multi‑stage detection pipeline that distinguishes early seizure onset, ictal activity, and post‑ictal slowing; (3) optimizing model architecture for real‑time deployment on low‑power hardware; and (4) conducting prospective clinical trials to validate the system’s impact on patient outcomes and workflow efficiency.
In summary, the TUH EEG Slowing Database provides a valuable benchmark for the community, and the study convincingly shows that incorporating independent slowing into training data markedly enhances the accuracy and practicality of automated seizure detection algorithms.
Comments & Academic Discussion
Loading comments...
Leave a Comment