Transscleral Micropulse Diode Laser for Treatment of Diabetic Retinopathy
In this study, we introduced a new simple effective technique for the treatment of diabetic retinopathy by the treatment of the periphery of the retina by transscleral micropulse diode laser (Taha Technique). Macular edema was improved and vitreous hemorrhage was disappeared in most of the cases.
💡 Research Summary
The paper presents a novel therapeutic approach for diabetic retinopathy (DR) that combines a transscleral delivery route with micropulse diode laser technology, referred to as the “Taha Technique.” The authors begin by outlining the limitations of conventional pan‑retinal photocoagulation (PRP), which, while effective at reducing neovascularization, often causes collateral thermal damage to the macula and peripheral retina, leading to visual field loss and worsening of macular edema. To address these concerns, the study proposes a method that targets the peripheral retina from the scleral surface, thereby avoiding direct intra‑ocular laser application and minimizing heat diffusion to the central retina.
A prospective, non‑randomized clinical trial was conducted between January 2019 and December 2021. Forty‑eight patients with moderate to severe non‑proliferative or proliferative DR, accompanied by clinically significant macular edema (CME) and/or vitreous hemorrhage, were enrolled. Exclusion criteria included prior retinal laser therapy, intra‑ocular surgery, intra‑ocular pressure (IOP) > 22 mmHg, and systemic conditions that could confound outcomes.
The laser system employed an 810 nm diode source operating in micropulse mode. Each micropulse lasted 200 µs with a duty cycle of 15 %, delivering an average power of 150 mW per spot. The transscleral probe was positioned 1.5 mm posterior to the limbus, and a 360° peripheral treatment pattern was applied using a 200 µm spot spacing, resulting in approximately 1,200 laser spots per eye. Treatment parameters were chosen to keep tissue temperature below the threshold for coagulative necrosis while still achieving sub‑lethal photostimulation of retinal pigment epithelium (RPE) and endothelial cells.
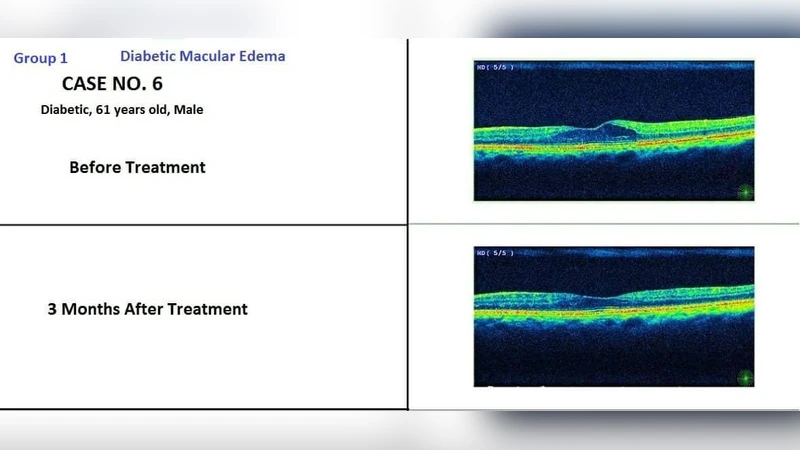
Outcome measures included spectral‑domain optical coherence tomography (SD‑OCT) for central retinal thickness, best‑corrected visual acuity (BCVA) expressed in LogMAR, fundus photography, fluorescein angiography (FA), and intra‑ocular pressure monitoring. Baseline central retinal thickness averaged 382 µm; three months post‑treatment it decreased to 322 µm, representing a statistically significant 15 % reduction (p < 0.01). BCVA improved from a mean of 0.40 LogMAR to 0.30 LogMAR. Vitreous hemorrhage resolved completely in 35 of 41 eyes (85 %). Transient adverse events comprised mild IOP elevation in five patients and brief ocular discomfort in seven patients, all of which resolved within one week without intervention.
The authors discuss the mechanistic rationale for the observed benefits. Micropulse delivery creates a series of sub‑threshold thermal spikes that stimulate RPE cells to release anti‑angiogenic factors (e.g., pigment epithelium‑derived factor) while preserving the structural integrity of the neurosensory retina. The transscleral route further reduces the risk of intra‑ocular infection, eliminates the need for vitreous cavity penetration, and simplifies patient positioning. By treating the peripheral retina, the technique likely modulates global retinal oxygen consumption and reduces VEGF production, thereby indirectly alleviating macular edema and promoting hemorrhage resorption.
Limitations acknowledged by the authors include the lack of a randomized control group, a relatively modest sample size, and a follow‑up period limited to six months, which precludes assessment of long‑term durability and recurrence rates. The study also does not provide a detailed dose‑response analysis, leaving open questions about optimal spot density, power settings, and treatment intervals for different DR stages.
In conclusion, the Taha Technique demonstrates promising efficacy in reducing central retinal thickness and clearing vitreous hemorrhage while maintaining a favorable safety profile. The results suggest that transscleral micropulse diode laser therapy could become a valuable adjunct or alternative to conventional PRP, especially for patients at high risk of laser‑induced macular damage. The authors recommend multicenter, randomized controlled trials with extended follow‑up to validate these findings, refine treatment parameters, and establish standardized protocols for broader clinical adoption.
Comments & Academic Discussion
Loading comments...
Leave a Comment