Newborn skin reflection: Proof of concept for a new approach for predicting gestational age at birth. A cross-sectional study
Current methods to assess the gestational age during prenatal care or at birth are a global challenge. Disadvantages, such as low accessibility, high costs, and imprecision of clinical tests and ultrasonography measurements, may compromise health decisions at birth, based on the gestational age. Newborns organs and tissues can indirectly indicate their physical maturity, and we hypothesized that evolutionary changes in their skin, detected using an optoelectronic device meter, may aid in estimating the gestational age. This study analyzed the feasibility of using newborn skin reflectance to estimate the gestational age at birth noninvasively. A cross-sectional study evaluated the skin reflectance of selected infants, preferably premature, at birth. The first-trimester ultrasound was the reference for gestational age. A prototype of a new noninvasive optoelectronic device measured the backscattering of light from the skin, using a light emitting diode at wavelengths of 470 nm, 575 nm, and 630 nm. Univariate and multivariate regression analysis models were employed to predict gestational age, combining skin reflectance with clinical variables for gestational age estimation. The gestational age at birth of 115 newborns from 24.1 to 41.8 weeks of gestation correlated with the light at 630 nm wavelength reflectance 3.3 mm/6.5 mm ratio distant of the sensor, at the forearm and sole . The best-combined variables to predict the gold standard gestational age at birth was the skin reflectance at wavelengths of 630 nm and 470 nm in combination with birth weight, phototherapy, and adjusted to include incubator stay, and sex. The main limitation of the study is that it was very specific to the premature population we studied and needs to be studied in a broader spectrum of newborns.
💡 Research Summary
The paper addresses the persistent global challenge of accurately determining gestational age (GA) at birth, a key factor influencing perinatal care decisions. Conventional methods—first‑trimester ultrasound, maternal recall of last menstrual period, and clinical scoring systems—are limited by cost, accessibility, and variable precision, especially in low‑resource settings. The authors hypothesized that the structural and biochemical maturation of newborn skin, which evolves predictably throughout gestation, could be captured non‑invasively through optical back‑scattering measurements.
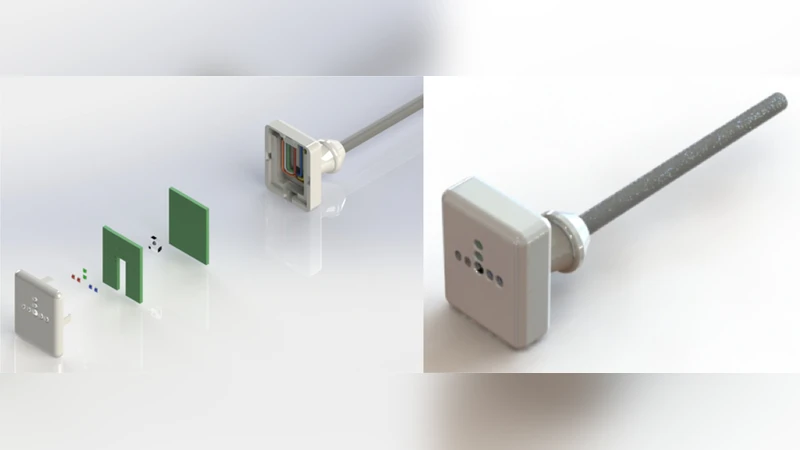
To test this, a prototype optoelectronic device was built that emits light‑emitting diodes (LEDs) at three wavelengths: 470 nm (blue), 575 nm (green), and 630 nm (red). The sensor records back‑scattered light at two fixed distances from the skin (3.3 mm and 6.5 mm), allowing calculation of a distance‑ratio reflectance for each wavelength. Measurements were taken on the forearm and the sole of 115 newborns whose GA ranged from 24.1 to 41.8 weeks, as established by first‑trimester ultrasound (the gold standard). The cohort was intentionally enriched for preterm infants to maximize the dynamic range of skin maturation.
Univariate regression identified the 630 nm reflectance ratio (3.3 mm/6.5 mm) on both sites as the strongest single predictor of GA (Pearson r ≈ 0.71). The 470 nm signal contributed modestly, while the 575 nm wavelength showed the weakest association. Multivariate linear regression then combined the two most informative optical variables (630 nm ratio and 470 nm absolute reflectance) with four clinical covariates: birth weight, phototherapy exposure, incubator stay, and infant sex. The final model achieved an adjusted R² of 0.78, a mean absolute error of 1.2 weeks, and a root‑mean‑square error of 1.5 weeks—substantially better than models using only clinical data or only optical data.
Key insights include: (1) red‑light back‑scatter is highly sensitive to dermal thickness and collagen content, both of which increase with gestational maturity; (2) the distance‑ratio metric normalizes for surface curvature and pressure effects, enhancing reproducibility; (3) integrating simple clinical variables refines the prediction, suggesting that skin optics capture complementary information rather than replace existing measures.
The study’s limitations are noteworthy. The sample is skewed toward preterm infants, limiting generalizability to term populations. All participants were recruited from a single tertiary center, with limited ethnic and skin‑pigmentation diversity, which may affect optical properties. Device calibration, inter‑operator variability, and environmental lighting were not systematically evaluated, raising questions about robustness in field conditions.
Future work should (a) validate the approach in larger, multi‑center cohorts encompassing a full spectrum of gestational ages and ethnicities; (b) explore non‑linear modeling techniques (e.g., random forests, neural networks) that could capture complex interactions among wavelengths, distances, and clinical factors; and (c) develop a rugged, low‑cost version of the sensor suitable for use in low‑resource birth settings.
In conclusion, the authors demonstrate a proof‑of‑concept that newborn skin reflectance, measured with a simple handheld optoelectronic device, can estimate gestational age with clinically useful accuracy. If refined and validated, this technology could become a valuable adjunct to existing GA assessment tools, particularly where ultrasound is unavailable or prohibitively expensive, thereby improving neonatal risk stratification and guiding timely interventions worldwide.
Comments & Academic Discussion
Loading comments...
Leave a Comment