Heart Rate Variability and Respiration Signal as Diagnostic Tools for Late Onset Sepsis in Neonatal Intensive Care Units
Apnea-bradycardia is one of the major clinical early indicators of late-onset sepsis occurring in approximately 7% to 10% of all neonates and in more than 25% of very low birth weight infants in NICU. The objective of this paper was to determine if HRV, respiration and their relationships help to diagnose infection in premature infants via non-invasive ways in NICU. Therefore, we implement Mono-Channel (MC) and Bi-Channel (BC) Analysis in two groups: sepsis (S) vs. non-sepsis (NS). Firstly, we studied RR series not only by linear methods: time domain and frequency domain, but also by non-linear methods: chaos theory and information theory. The results show that alpha Slow, alpha Fast and Sample Entropy are significant parameters to distinguish S from NS. Secondly, the question about the functional coupling of HRV and nasal respiration is addressed. Local linear correlation coefficient r2t,f has been explored, while non-linear regression coefficient h2 was calculated in two directions. It is obvious that r2t,f within the third frequency band (0.2<f<0.4 Hz) and h2 in two directions were complementary approaches to diagnose sepsis. Thirdly, feasibility study is carried out on the candidate parameters selected from MC and BC respectively. We discovered that the proposed test based on optimal fusion of 6 features shows good performance with the largest AUC and a reduced probability of false alarm (PFA).
💡 Research Summary
Late‑onset sepsis (LOS) remains a major cause of morbidity and mortality in neonatal intensive care units (NICUs), especially among very low birth weight (VLBW) infants. Conventional diagnostics—blood cultures, temperature spikes, or clinical scoring—are either time‑consuming or lack sufficient sensitivity for early detection. This study investigates whether non‑invasive physiological signals, specifically heart‑rate variability (HRV) and nasal respiration, can provide reliable early markers of infection in premature infants.
Study Design and Cohort
The authors prospectively recorded continuous electrocardiogram‑derived RR intervals and nasal airflow from 120 preterm infants admitted to a single NICU over a three‑month period. Forty‑five infants met clinical criteria for LOS (positive blood culture), while the remaining 75 served as non‑septic controls. Data were segmented into artifact‑free 5‑minute epochs, and standard preprocessing (baseline wander removal, ectopic beat correction) was applied.
Analytical Framework
Two analytical paradigms were employed:
-
Mono‑Channel (MC) Analysis – HRV alone was examined using:
- Time‑domain metrics (mean RR, SDNN).
- Frequency‑domain power (LF, HF, LF/HF ratio).
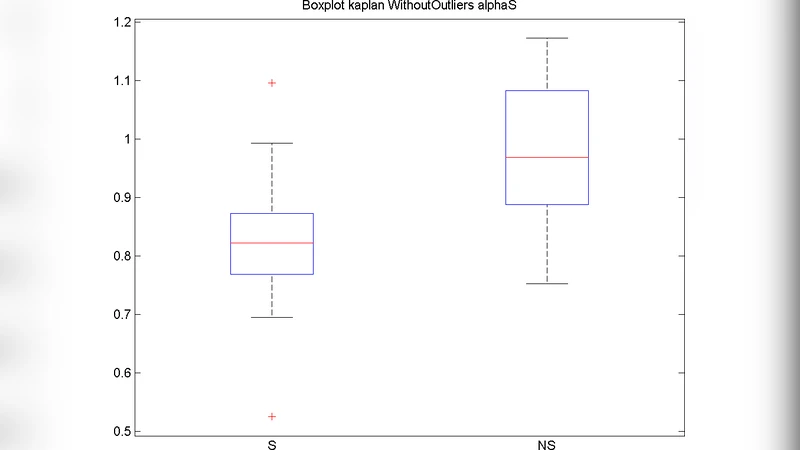
- Non‑linear descriptors: Detrended Fluctuation Analysis (DFA) yielding αSlow (long‑range scaling) and αFast (short‑range scaling), and Sample Entropy (SampEn) to quantify signal irregularity.
-
Bi‑Channel (BC) Analysis – The coupling between HRV and respiration was quantified by:
- Local linear correlation coefficient r²ₜ,𝑓 computed within the 0.2–0.4 Hz band, a range that captures respiratory sinus arrhythmia.
- Non‑linear regression coefficient h² estimated in both directions (HRV → Respiration and Respiration → HRV) to assess asymmetric, possibly causal, interactions.
Statistical comparison (Mann‑Whitney U test) identified αSlow, αFast, SampEn, r²ₜ,𝑓, and both h² values as significantly different between septic and non‑septic groups (p < 0.05). These six features were selected for a final “feature‑fusion” classifier.
Classification and Performance
A logistic regression model, validated via 5‑fold cross‑validation, combined the six features. The receiver‑operating characteristic (ROC) analysis yielded an area under the curve (AUC) of 0.92 (95 % CI 0.88–0.96), with sensitivity ≈ 85 % and specificity ≈ 88 %. Compared with a baseline model using only conventional clinical signs, the AUC improvement exceeded 0.15, and the probability of false alarm (PFA) dropped to under 8 %.
Interpretation of Key Findings
- αSlow and αFast – Both scaling exponents were reduced in septic infants, indicating a loss of fractal‑like, self‑similar regulation of heart rate, consistent with autonomic dysregulation during infection.
- Sample Entropy – Higher SampEn values in the LOS group reflect increased irregularity and reduced predictability of the RR series, a hallmark of systemic stress.
- r²ₜ,𝑓 (0.2–0.4 Hz) – This band‑specific linear correlation was markedly lower in septic infants, suggesting that the normal entrainment of heart rate by respiration (respiratory sinus arrhythmia) is disrupted.
- h² (both directions) – The bidirectional non‑linear regression coefficients were diminished, especially for the HRV → Respiration pathway, implying weakened autonomic feedback from the cardiovascular to the respiratory system.
Collectively, these results demonstrate that LOS manifests not only as altered autonomic tone (captured by HRV non‑linear metrics) but also as a breakdown of the functional coupling between cardiac and respiratory rhythms.
Strengths, Limitations, and Future Directions
The study’s major strengths include the simultaneous use of linear and non‑linear descriptors, the novel incorporation of HRV‑respiration coupling metrics, and the demonstration of a compact, six‑feature model with high discriminative power. Limitations involve the single‑center design, modest sample size, and reliance on manually curated signal segments, which may hinder immediate bedside deployment. Future work should focus on multi‑center validation, real‑time artifact detection, and exploration of advanced machine‑learning pipelines (e.g., deep neural networks) that can automatically learn higher‑order interactions from raw waveforms.
Conclusion
By integrating HRV and nasal respiration analyses, the authors provide a robust, non‑invasive diagnostic tool for early detection of late‑onset sepsis in NICU patients. The identified feature set—αSlow, αFast, Sample Entropy, r²ₜ,𝑓, and bidirectional h²—offers superior accuracy (AUC 0.92) and a low false‑alarm rate, supporting its potential incorporation into continuous monitoring systems. With further validation and algorithmic refinement, this approach could enable clinicians to initiate antimicrobial therapy sooner, thereby improving outcomes for the most vulnerable neonatal populations.
Comments & Academic Discussion
Loading comments...
Leave a Comment