Modeling In vivo Wireless Path Loss
Our long-term research goal is to model the in vivo wireless channel. As a first step towards this goal, in this paper we performed in vivo path loss measurements at 2.4GHz and make a comparison with
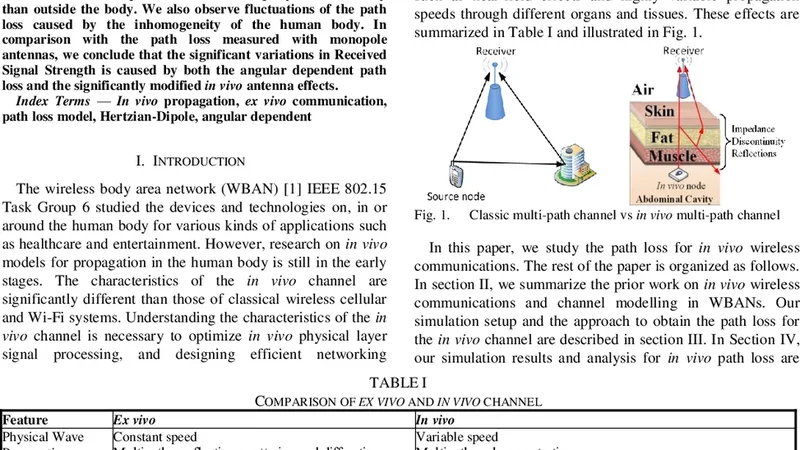
Our long-term research goal is to model the in vivo wireless channel. As a first step towards this goal, in this paper we performed in vivo path loss measurements at 2.4GHz and make a comparison with free space path loss. We calculate the path loss by using the electric field radiated by a Hertzian-Dipole located inside the abdominal cavity. The simulations quantify and confirm that the path loss falls more rapidly inside the body than outside the body. We also observe fluctuations of the path loss caused by the inhomogeneity of the human body. In comparison with the path loss measured with monopole antennas, we conclude that the significant variations in Received Signal Strength is caused by both the angular dependent path loss and the significantly modified in vivo antenna effects.
💡 Research Summary
The paper presents an initial step toward a comprehensive model of the in‑vivo wireless channel by measuring and analyzing path loss at the 2.4 GHz ISM band inside a human abdominal cavity. Using full‑wave electromagnetic simulations, the authors place a Hertzian‑dipole source within a high‑resolution anatomical model and compute the electric field at various observation points. Path loss (PL) is derived from the ratio of transmitted to received field strength expressed in decibels, allowing a direct comparison with free‑space loss under identical geometric conditions.
Key findings are as follows. First, the in‑vivo PL is substantially higher than free‑space loss, typically 20–30 dB greater for the same transmitter‑receiver separation. This steep attenuation is attributed to the high permittivity and conductivity of biological tissues (muscle, fat, organs), which absorb and scatter the electromagnetic wave far more aggressively than air. Second, the PL exhibits pronounced angular dependence. When the dipole radiates toward tissue interfaces—particularly the muscle‑fat boundary—the mismatch in impedance causes rapid fluctuations of up to ±5 dB, highlighting the heterogeneous nature of the human body as a dominant factor in signal variability. Third, the study contrasts the Hertzian‑dipole results with prior measurements using monopole antennas. While monopoles are often assumed to have a relatively stable radiation pattern in free space, the in‑vivo environment dramatically alters the antenna’s input impedance and radiation efficiency. Consequently, the observed variations in received signal strength (RSSI) are not solely distance‑based but stem from a combination of angular‑dependent loss and the altered antenna characteristics inside tissue.
Methodologically, the work employs a voxel‑based human model with tissue‑specific dielectric parameters taken from the IT’IS database. The simulation domain includes perfectly matched layers to suppress reflections, and a parametric sweep over polar and azimuthal angles provides a dense mapping of PL across the surrounding space. The authors also perform a baseline free‑space simulation using the same dipole geometry to isolate the contribution of the body’s material properties.
From a system‑design perspective, the results suggest several practical guidelines. (1) Antenna placement and orientation must be optimized for the specific anatomical region to mitigate angular loss peaks. (2) Channel models for implantable or ingestible devices should incorporate angle‑dependent attenuation terms rather than relying on simple distance‑only path‑loss exponents. (3) Matching networks or low‑loss antenna designs tailored to the surrounding tissue’s permittivity are essential to preserve radiation efficiency. (4) Link‑budget calculations for in‑vivo communication should allocate an additional 20–30 dB margin to account for tissue‑induced loss.
The authors conclude that the rapid decay of signal strength inside the body, together with the observed fluctuations caused by tissue heterogeneity, confirms that both angular path loss and modified in‑vivo antenna behavior are responsible for the significant RSSI variations reported in earlier monopole‑based studies. This work lays the groundwork for more accurate, anatomy‑aware channel models and informs the design of reliable wireless medical devices operating within the human body. Future research directions include experimental validation with animal or cadaver studies, extension to other frequency bands (e.g., 433 MHz, 5 GHz), exploration of dynamic physiological effects such as breathing and blood flow, and the development of adaptive antenna systems capable of real‑time impedance tuning within tissue.
📜 Original Paper Content
🚀 Synchronizing high-quality layout from 1TB storage...