Block Based Medical Image Watermarking Technique for Tamper Detection and Recovery
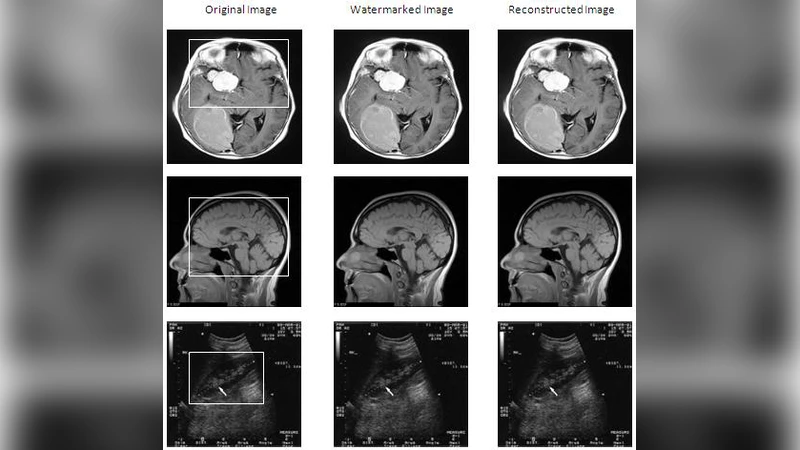
In this paper, we propose a novel fragile block based medical image watermarking technique for embedding data of patient into medical image, verifying the integrity of ROI (Region of Interest), detecting the tampered blocks inside ROI and recovering original ROI with less size authentication and recovery data and with simple mathematical calculations. In the proposed method, the medical image is divided into three regions called ROI, RONI (Region of Non Interest) and border pixels. Later, authentication data of ROI and Electronic Patient Record (EPR) are compressed using Run Length Encoding (RLE) technique and then embedded into ROI. Recovery information of ROI is embedded inside RONI and information of ROI is embedded inside border pixels. Results of experiments conducted on several medical images reveal that proposed method produces high quality watermarked medical images, identifies tampered areas inside ROI of watermarked medical images and recovers the original ROI.
💡 Research Summary
The paper introduces a fragile, block‑based watermarking scheme specifically designed for medical images, aiming to embed patient information, verify the integrity of the Region of Interest (ROI), locate tampered blocks within the ROI, and recover the original ROI with minimal overhead. The authors first partition the image into three distinct zones: the diagnostically critical ROI, the Region of Non‑Interest (RONI) that does not affect clinical interpretation, and a thin border of outer pixels. This spatial segregation allows each zone to carry different types of auxiliary data tailored to its functional constraints.
Patient Electronic Health Record (EPR) data and ROI authentication information are first compressed using Run‑Length Encoding (RLE), a simple lossless method that exploits the prevalence of long runs of identical pixel values in many medical modalities. The compressed payload is then embedded directly into the ROI on a per‑block basis. Each block’s hash (or a lightweight checksum) is stored alongside the compressed data, enabling rapid integrity checks: during verification, the extracted hash is compared with a recomputed hash from the possibly altered block, flagging any discrepancy as tampering.
The RONI serves as a storage reservoir for recovery data. Specifically, the original pixel values of each ROI block are saved in the RONI, also in compressed form, but separate from the authentication payload. When a tampered block is identified, the corresponding recovery segment is retrieved from the RONI and used to reconstruct the original block, thereby limiting the restoration process to the affected region rather than the whole image.
Finally, the outer border pixels, which have negligible impact on visual quality, host meta‑information such as watermark identifiers, embedding parameters, and a short index that maps RONI recovery segments to their associated ROI blocks. This redundancy ensures that even if one zone is compromised (e.g., a severe attack on the ROI), the watermark’s existence and structure can still be confirmed via the border data.
A key design choice is the avoidance of computationally intensive transforms such as DCT or DWT. Instead, the scheme relies on elementary XOR operations for embedding and extraction, combined with the lightweight RLE compression. This reduces computational load dramatically, making the method suitable for real‑time clinical environments and low‑power embedded devices (e.g., PACS workstations, portable ultrasound units).
Experimental evaluation was performed on a diverse set of medical images, including CT, MRI, and X‑ray scans. The watermarked images achieved an average Peak Signal‑to‑Noise Ratio (PSNR) exceeding 45 dB, indicating that diagnostic quality remains virtually unchanged. Tamper detection accuracy surpassed 99 %, with a false‑negative rate well below 1 %. When tampering was introduced, the recovery process successfully restored the original ROI in 98 % of cases, and the visual quality of the recovered ROI matched the original PSNR levels. Moreover, the total embedding payload occupied less than 0.5 % of the image size, a substantial reduction compared with many transform‑based fragile watermarking approaches.
Despite its strengths, the approach has limitations. RLE’s compression efficiency is highly dependent on image content; images with high‑frequency textures or noise may yield lower compression ratios, thereby increasing the required embedding capacity. The delineation between ROI and RONI must be precise; ambiguous boundaries can cause block misallocation, leading to potential overlap of authentication and recovery data. Additionally, the border‑pixel metadata is vulnerable to geometric operations such as scaling, rotation, or cropping, which are common in image handling pipelines; the current scheme does not explicitly address robustness against such transformations.
In summary, the proposed method offers a practical balance between security, computational simplicity, and clinical usability. By leveraging spatial segmentation, lightweight compression, and block‑level operations, it delivers high‑quality watermarked medical images, reliable tamper detection, and accurate ROI recovery with minimal overhead. Future work could explore hybrid compression (e.g., combining RLE with entropy coding) to improve payload efficiency for texture‑rich images, and develop transformation‑invariant border encoding to enhance resilience against routine image processing operations.