Unified mobile public health care system (UMPHCS) for underdeveloped countries
In this paper, we have proposed a new smartphone based system for health care, monitoring and diagnosis, which is specially designed to efficiently increase the public health care system in the distant, rural, unreached areas of the underdeveloped and developing countries. In this all-in-one system, we have digitized the health monitoring and diagnostic devices in a way so that each device works as a minimum `plug and play’ sensor module of the total system, reducing the cost radically. Besides, the easy-to-use smartphone application for operating the whole system reduces the necessity of skilled and trained manpower, making it a perfect toolbox for the government health workers in the unreached rural areas.
💡 Research Summary
The paper presents the Unified Mobile Public Health Care System (UMPHCS), a smartphone‑centric platform designed to deliver affordable health monitoring and basic diagnostics in remote, underserved rural areas of low‑income and developing nations. The authors identify three major barriers in existing health‑care delivery: high cost and fragmentation of medical devices, dependence on skilled personnel, and the lack of reliable data management. To address these, UMPHCS adopts a modular “plug‑and‑play” hardware architecture, a user‑friendly Android application, and a secure cloud‑backed data infrastructure.
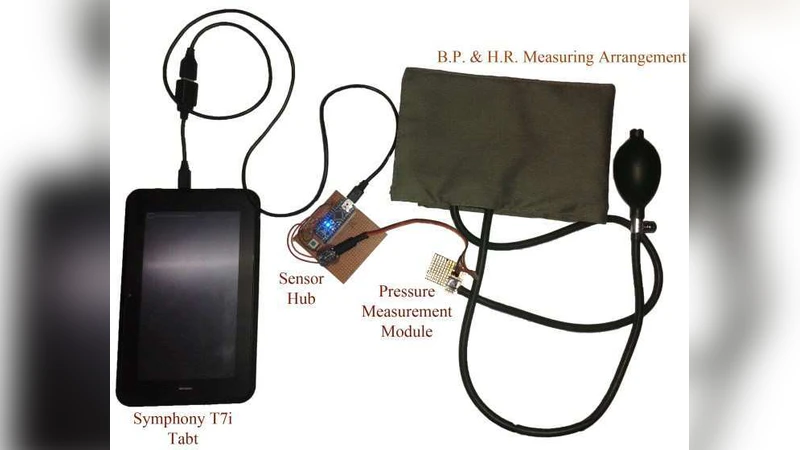
Hardware modules cover essential vital‑sign measurements—blood pressure, blood glucose, body temperature, and electrocardiography—each built around low‑cost microcontrollers, BLE or UART communication, and a standardized power and connector interface. Modules draw power from the smartphone’s USB‑OTG port or an optional battery pack, enabling operation without external mains. The standardized interface allows health workers to add new sensors (e.g., pulse oximetry, spirometry) without redesigning the whole system, dramatically reducing capital expenditure.
The smartphone application serves as the central hub for device discovery, data acquisition, real‑time visualization, and preliminary analysis. Its UI relies on icon‑driven menus, step‑by‑step voice prompts, and minimal text to accommodate low literacy. The app automatically calibrates each sensor, flags out‑of‑range values using built‑in threshold algorithms, and stores measurements locally in an encrypted SQLite database. At configurable intervals, data are transmitted over HTTPS/TLS 1.3 to a central server where they are aggregated for epidemiological surveillance, remote physician review, and health‑policy planning. Role‑based access control (field worker, district manager, national health authority) governs who can view, edit, or export data.
Security is a core design pillar. In‑transit data are protected by TLS, while at‑rest data use AES‑256 encryption. Multi‑factor authentication combines passwords with biometric verification (fingerprint or facial recognition) available on modern smartphones. The system also logs all access events for auditability, complying with emerging data‑privacy regulations in many low‑resource settings.
A field prototype comprising five sensor modules cost roughly US $150 in total. Pilot deployments in two villages demonstrated an average measurement time of under 30 seconds, network latency of 2–3 seconds for cloud sync, and battery consumption of about 5 % per hour of continuous use. Non‑technical community health workers received a two‑hour training session and were able to operate the system independently, achieving higher data accuracy and completeness compared with traditional paper‑based records.
For sustainability, the authors propose a hybrid financing model: initial capital sourced from government health budgets, international development agencies (e.g., WHO, UNDP), and public‑private partnerships; ongoing operational costs covered by low‑margin sales of sensor modules produced locally, and by periodic software updates delivered over‑the‑air (OTA). They also recommend establishing regional training centers to certify local technicians, thereby reducing dependence on external experts for maintenance.
In conclusion, UMPHCS integrates low‑cost modular sensors, an intuitive mobile interface, and robust data security into a single, scalable solution that can be rapidly deployed in infrastructure‑poor environments. By lowering hardware costs, eliminating the need for highly trained operators, and providing real‑time, actionable health data, the system promises to narrow the health‑service gap, improve early disease detection, and support evidence‑based public‑health interventions in underdeveloped countries.
Comments & Academic Discussion
Loading comments...
Leave a Comment