Thorotrast and in vivo thorium dioxide: numerical simulation of 30 years of alpha radiation absorption by the tissues near a large compact source
Background: The epidemiology of the slightly radioactive contrast agent named Thorotrast presents a very long latency period between the injection and the development of the related pathologies. It is an example of the more general problem posed by a radioactive internal contaminant whose effects are not noteworthy in the short term but become dramatic in the long period. A point that is still to be explored is fluctuations (in space and time) in the localized absorption of radiation by the tissues. Methods: A Monte Carlo simulation code has been developed to study over a 30 year period the daily absorption of alpha radiation by micrometer sized portions of tissue placed at a distance of 0-100 micrometers from a model source, that approximates a compact thorium dioxide source in liver or spleen whose size is larger or equal to 20 micrometers. The biological depletion of the daughter nuclei of the thorium series is taken into account. The initial condition assumes chemically purified natural thorium. Results: Most of the absorbed dose is concentrated in a 25 micrometer thick layer of tissue, adjacent to the source boundary. Fluctuations where a target region with a volume of 1 cube micrometer is hit by 3-5 alpha particles in a day or in a shorter period of time are relevant in a 1-10 micrometer thick layer of tissue adjacent to the source boundary, where their frequency is larger than the Poisson law prediction.
💡 Research Summary
The paper investigates the long‑term radiobiological effects of Thorotrast, a thorium dioxide (ThO₂) contrast agent historically used in radiology, by focusing on the spatial and temporal fluctuations of α‑particle dose deposition in tissues adjacent to a compact source. Thorotrast particles, typically 20 µm or larger, accumulate in the liver and spleen and remain essentially unchanged for decades, leading to a latency period of 30–40 years before malignancies appear. Conventional risk assessments based on average dose rates cannot explain this delayed onset, prompting the authors to explore dose heterogeneity at the micrometer scale.
A Monte‑Carlo code was developed to simulate 30 years (≈10⁴ days) of α‑particle emission from a source that mimics a compact ThO₂ aggregate. The source is modeled as an infinite half‑space with a flat, well‑defined boundary; tissue is represented on the opposite side. The simulation tracks individual nuclear decays in the ²³²Th and ²²⁸Th decay chains, including the short‑lived daughters (²²⁸Ra → ²²⁴Ra → ²²⁰Rn → ²¹⁶Po, etc.). Decay times are generated from exponential distributions, and a “biological depletion” factor is applied to account for the removal of daughter nuclei from the source by physiological processes (rates taken from literature for liver and spleen). Each α‑particle’s initial energy (4–6 MeV for the majority of emissions) and direction are sampled, and its trajectory is propagated through ThO₂ and tissue using stopping‑power data, with a spatial resolution of 0.1–0.5 µm and a temporal resolution of 15 minutes.
The key findings are:
-
Dose Gradient – The majority (≈80 %) of the absorbed dose is confined within a 25 µm thick layer of tissue directly adjacent to the source boundary. Beyond 25 µm the dose drops sharply to negligible levels because the α‑particle range in soft tissue is only 40–60 µm.
-
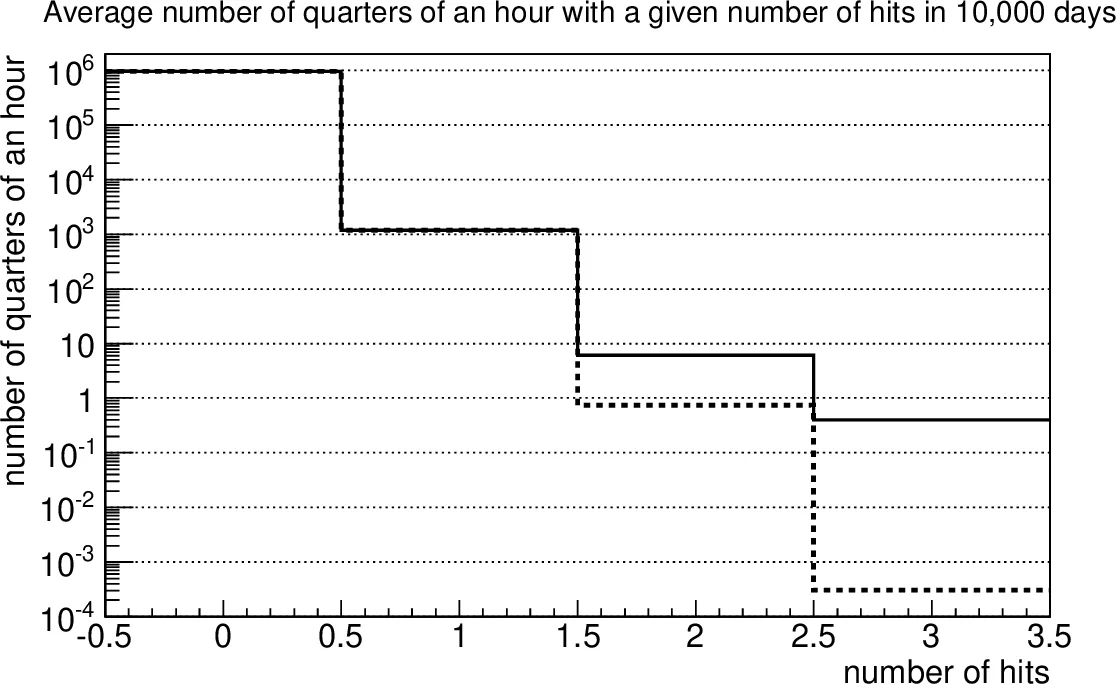
Fluctuation Hot‑Spots – In the 1–10 µm thick “near‑boundary” zone, a 1 µm³ tissue voxel experiences 3–5 α‑particle hits in a single day far more often than predicted by a Poisson distribution with the same mean (λ≈0.02–0.05). The observed frequency can be an order of magnitude higher, indicating clustering of decays within a single decay chain (e.g., the rapid succession of ²²⁸Th → ²²⁴Ra → ²²⁰Rn → ²¹⁶Po). These clusters produce short‑duration, high‑dose “bursts” lasting from minutes to a few hours.
-
Effect of Source Geometry – For a given mass of ThO₂, a compact aggregate maximizes self‑absorption, reducing the total emitted dose but concentrating it at the tissue interface. A dispersed distribution of micro‑fragments would increase the overall emitted dose but spread it more uniformly, lowering the peak dose in any microscopic region.
-
Biological Depletion – Incorporating the probability that daughter nuclei are removed from the source before they can decay reduces the long‑term activity of the ²³²Th chain to a quasi‑steady state after ~10 years, matching epidemiological observations that activity declines in the first decade and then stabilizes.
The authors argue that these microscopic, high‑dose bursts are biologically significant because α‑particles deposit energy densely over sub‑micron tracks, causing complex DNA double‑strand breaks. A tissue voxel receiving several hits in a short interval may experience a “critical lesion” that overwhelms cellular repair mechanisms, potentially initiating carcinogenesis. This mechanism provides a plausible explanation for the long latency of Thorotrast‑related cancers, which cannot be captured by models that average dose over macroscopic volumes or long time spans.
The paper concludes that risk assessment for internal α‑emitters such as Thorotrast must incorporate spatial‑temporal dose fluctuations, source micro‑architecture, and biological depletion processes. Future work should aim at detailed histological mapping of Thorotrast deposits, validation of the Monte‑Carlo predictions with microdosimetric measurements, and integration of these fluctuation‑aware dose metrics into epidemiological models to improve predictions of cancer risk for patients exposed to long‑lived internal radionuclides.
Comments & Academic Discussion
Loading comments...
Leave a Comment