Long Brief Pulse Method for Pulse-wave modified Electroconvulsive Therapy
Modified-Electroconvulsive Therapy (m-ECT) is administered for the treatment of various psychiatric disorders. The Seizure Generalization Hypothesis holds that propagation of the induced seizure throughout the whole brain is essential for the effective ECT intervention. However, we encounter many clinical cases where, due to high thresholds, seizure is not induced by the maximum dose of electrical charge. Some studies have indicated that the ultrabrief pulse method, in which pulse width is less than 0.5millisecond (ms), is more effective at inducing seizure than conventional brief pulse (0.5ms-2.0ms). Contrary to the studies, we experienced a case of schizophrenia in which m-ECT with 1.0 and 1.5 ms width pulse (referred to as ’long’ brief pulse as 0.5ms width pulse is the default in Japan) succeeded in inducing seizure, whereas ultrabrief pulse failed to induce seizure. This case is described in detail. Moreover, we discuss the underlying mechanism of this phenomenon.
💡 Research Summary
The paper reports a single‑patient case that challenges the prevailing view that ultrabrief pulse widths (≤0.5 ms) are universally superior for inducing seizures during modified electroconvulsive therapy (m‑ECT). The authors begin by outlining the “Seizure Generalization Hypothesis,” which posits that successful ECT requires the induced seizure to propagate throughout the entire brain. While many recent studies have shown that ultrabrief pulses reduce cognitive side‑effects and often lower the electrical charge needed to trigger a seizure, clinicians still encounter “high‑threshold” patients in whom even the maximum permissible charge fails to elicit a seizure.
In the presented case, a 45‑year‑old man with treatment‑resistant schizophrenia underwent a series of m‑ECT attempts. Initial trials using the standard 0.5 ms pulse (the default in Japan) at the maximum charge (≈900 mC) produced no electroencephalographic or motor seizure activity. When the pulse width was increased to 1.0 ms, the patient experienced two consecutive generalized seizures, accompanied by marked improvement in both positive and negative schizophrenic symptoms. A further trial with a 1.5 ms pulse also reliably induced seizures, and the cognitive side‑effects (primarily short‑term memory disturbances) were not appreciably worse than those reported for ultrabrief protocols.
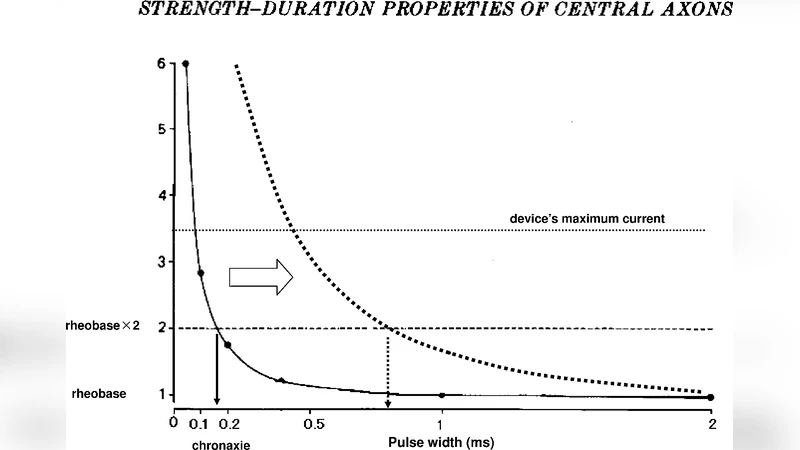
The authors analyze this paradox from both biophysical and clinical perspectives. First, longer pulse widths deliver more charge per pulse (Q = I × t), which can overcome a high seizure threshold by providing sufficient depolarizing current to neuronal membranes. Second, the impedance of brain tissue is not constant; it varies with pulse duration, and longer pulses may reduce the peak voltage required at the electrode‑brain interface, allowing a more uniform current spread. Third, pharmacological factors (e.g., antipsychotic‑induced ion‑channel modulation) and age‑related changes in neuronal excitability can blunt the responsiveness to ultrabrief pulses, making longer pulses a more effective stimulus in certain subpopulations.
Importantly, the paper emphasizes the trade‑off between seizure efficacy and cognitive side‑effects. While ultrabrief pulses are attractive for their neuroprotective profile, they are of limited value if they cannot reliably induce a seizure. Conversely, longer brief pulses may increase seizure yield without proportionally increasing adverse cognitive outcomes, especially when tailored to the individual’s physiological and pharmacological context. The authors therefore propose a “personalized pulse‑width strategy,” wherein clinicians assess seizure threshold, age, medication load, and possibly neuroimaging‑derived conductivity maps before selecting the optimal pulse width.
In conclusion, the authors argue that current ECT guidelines, which often fix the pulse width at 0.5 ms, may be overly restrictive. They call for systematic research—combining computational modeling of neuronal excitability, large‑scale clinical registries, and longitudinal cognitive assessments—to delineate the precise relationship between pulse width, seizure induction success, therapeutic efficacy, and side‑effect burden. Such data would enable evidence‑based, patient‑specific adjustments of pulse parameters, potentially improving outcomes for high‑threshold patients who are otherwise refractory to standard ultrabrief ECT protocols.
Comments & Academic Discussion
Loading comments...
Leave a Comment