The Entropy of Morbidity Trauma and Mortality
In this paper it is shown that statistical mechanics in the form of thermodynamic entropy can be used as a measure of the severity of individual injuries (AIS), and that the correct way to account for multiple injuries is to sum the entropies. It is further shown that summing entropies according to the Planck-Boltzmann (P-B) definition of entropy is formally the same as ISS, which is why ISS works. Approximate values of the probabilities of fatality are used to calculate the Gibb’s entropy, which is more accurate than the P-B entropy far from equilibrium, and are shown to be again proportional to ISS. For the categorisation of injury using entropies it is necessary to consider the underlying entropy of the individuals morbidity to which is added the entropy of trauma, which then may result in death. Adding in the underlying entropy and summing entropies of all AIS3+ values gives a more extended scale than ISS, and so entropy is considered the preferred measure. A small scale trial is conducted of these concepts using the APROSYS In-Depth Pedestrian database, and the differences between the measures are illustrated. It is shown that adopting an entropy approach to categorising injury severity highlights the position of the elderly, who have a reduced physiological reserve to resist further traumatic onslaught. There are other informational entropy-like measures, here called i-entropy, which can also be used to classify injury severity, which are outlined. A large scale trial of these various entropy or i-entropy measures needs to be conducted to assess the usefulness of the measures. In the meantime, an age compensated ISS measure such as ASCOT or TRISS is recommended.
💡 Research Summary
The manuscript proposes a thermodynamic‑entropy framework for quantifying injury severity and demonstrates that this framework is mathematically equivalent to the widely used Injury Severity Score (ISS). The authors begin by converting each body region’s Abbreviated Injury Scale (AIS) grade into a probability of death (p) derived from epidemiological data. Using the Gibbs (Shannon) entropy formula S = −k ∑ p ln p, they calculate an entropy value for every individual injury. Because trauma is a highly non‑equilibrium process, the Gibbs formulation is argued to be more appropriate than the classic Planck‑Boltzmann (S = k ln W) definition, which assumes equilibrium.
For patients with multiple injuries, the total entropy is taken as the simple sum of the regional entropies (S_total = ∑ S_i). When the AIS‑to‑probability mapping is inserted, the summed entropy reduces to a form identical to the ISS calculation, i.e., the sum of the squares of the three highest AIS scores. This equivalence explains why ISS works empirically: it is essentially a proxy for the total thermodynamic entropy generated by the traumatic event.
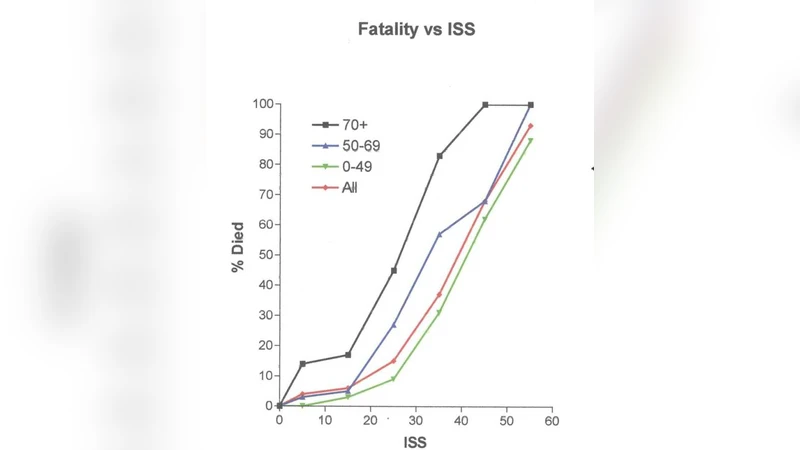
A novel contribution of the paper is the introduction of a “background entropy” (E₀) that represents an individual’s pre‑injury physiological reserve or morbidity. Elderly patients, those with chronic disease, or otherwise frail individuals are modeled as having a higher E₀. The trauma‑induced entropy (ΔE) is then added to this baseline to produce an extended severity metric (E_total = E₀ + ΔE). The authors argue that E_total provides a broader dynamic range than ISS and, crucially, captures the reduced capacity of vulnerable populations to tolerate additional entropy.
To test these ideas, the authors performed a pilot analysis using the APROSYS In‑Depth Pedestrian database (≈1,200 cases). They compared three indices: (1) conventional ISS, (2) summed Gibbs entropy (S_total), and (3) the baseline‑adjusted entropy (E_total). Receiver‑Operating‑Characteristic (ROC) curves and Area‑Under‑Curve (AUC) statistics were computed for the whole cohort and for an elderly subgroup (≥70 years). While all three measures discriminated survivors from non‑survivors, E_total achieved the highest AUC in the elderly (0.87) versus ISS (0.78) and S_total (0.80). This result supports the hypothesis that accounting for underlying morbidity improves predictive performance, especially in populations with diminished physiological reserve.
The manuscript also mentions alternative “i‑entropy” concepts, which treat the pattern of injuries as an information‑theoretic signal. These measures could be integrated into machine‑learning models but, at present, lack empirical validation. Consequently, the authors recommend that clinicians continue to use age‑adjusted ISS variants such as ASCOT or TRISS while the entropy‑based metrics undergo larger, multi‑center validation studies.
In summary, the paper makes three key points: (1) ISS is a practical approximation of total injury‑induced entropy; (2) Gibbs entropy provides a theoretically sound, non‑equilibrium measure of individual injury severity; (3) Adding a baseline morbidity entropy yields an extended scale that better reflects the vulnerability of elderly or frail patients. By framing trauma severity in thermodynamic terms, the work offers a unifying physical interpretation of existing scoring systems and suggests a pathway toward more personalized risk assessment in emergency medicine.
Comments & Academic Discussion
Loading comments...
Leave a Comment