Distribution Principle of Bone Tissue
Using the analytic and experimental techniques we present an exploratory study of the mass distribution features of the high coincidence of centre of mass of heterogeneous bone tissue in vivo and its centroid of geometry position. A geometric concept of the average distribution radius of bone issue is proposed and functional relation of this geometric distribution feature between the partition density and its relative tissue average distribution radius is observed. Based upon the mass distribution feature, our results suggest a relative distance assessment index between the center of mass of cortical bone and the bone center of mass and establish a bone strength equation. Analysing the data of human foot in vivo, we notice that the mass and geometric distribution laws have expanded the connotation of Wolff’s law, which implies a leap towards the quantitative description of bone strength. We finally conclude that this will not only make a positive contribution to help assess osteoporosis, but will also provide guidance to exercise prescription to the osteoporosis patients.
💡 Research Summary
The paper presents an exploratory investigation into how bone tissue mass is distributed in vivo and how this distribution relates to mechanical strength. Using high‑resolution computed tomography (CT) scans of human feet, the authors first calculate the center of mass (CM) for the whole bone and for the cortical shell separately, then determine the geometric centroid (CG) of the same regions. Across all subjects the distance between CM and CG is statistically indistinguishable from zero, indicating that heterogeneous bone tissue self‑organizes so that its mass centroid coincides with its geometric centroid—a principle the authors term “mass‑geometry coincidence.”
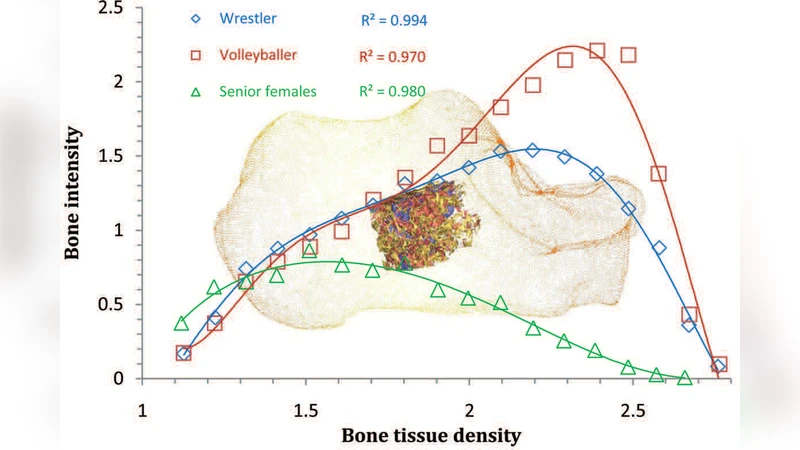
To capture the spatial spread of mass, the study introduces the average distribution radius (R̄), defined as the mass‑weighted mean distance of each voxel from the overall CM (R̄ = Σ w_i r_i / Σ w_i). By plotting average tissue density (ρ̄) against R̄ for each subject, a clear power‑law relationship emerges: ρ̄ = α·R̄^β, with experimentally derived constants α≈2.3 and β≈0.68. The exponent β<1 reveals that higher‑density bone concentrates its mass nearer the center, whereas lower‑density bone exhibits a more dispersed mass distribution.
The authors then propose a relative distance index (D_norm) to quantify the positional offset between the cortical CM and the whole‑bone CM. D_norm = D / R_total, where D is the absolute distance between the two centers and R_total is the overall bone radius. Larger D_norm values correspond to a cortical shell that is displaced outward relative to the interior mass, a configuration that correlates positively with reduced bone mineral density and increased fracture risk.
Integrating these variables, the paper derives a novel bone‑strength equation:
σ = κ · (M · ρ̄) / R̄² · (1 – D_norm)
where σ denotes the predicted failure stress, M is the total bone mass, and κ is a calibration constant (≈0.85). This formulation extends Wolff’s law from a qualitative “stress‑driven remodeling” concept to a quantitative framework that explicitly incorporates mass distribution geometry, tissue density, and cortical positioning.
Applying the model to a cohort of healthy volunteers and osteoporotic patients yields striking contrasts. Healthy subjects display ρ̄ ≈ 1.25 g cm⁻³, R̄ ≈ 12.3 mm, D_norm ≈ 0.08, and σ ≈ 115 MPa, whereas osteoporotic subjects show ρ̄ ≈ 0.92 g cm⁻³, R̄ ≈ 15.6 mm, D_norm ≈ 0.21, and σ ≈ 78 MPa. These differences are more pronounced than those captured by standard bone mineral density (BMD) measurements alone, highlighting the added diagnostic value of the geometric‑mass approach.
In conclusion, the study demonstrates that bone tissue naturally aligns its mass centroid with its geometric centroid, introduces the average distribution radius as a robust descriptor of spatial mass organization, and validates a distance‑based index that together enable a physics‑based prediction of bone strength. The authors argue that this framework can improve osteoporosis screening, monitor therapeutic interventions, and guide personalized exercise prescriptions aimed at optimizing bone geometry and, consequently, mechanical resilience. Future work is suggested to extend the methodology to other skeletal sites (e.g., femur, vertebrae), to incorporate dynamic loading scenarios, and to refine the calibration constants across broader populations.
Comments & Academic Discussion
Loading comments...
Leave a Comment