The excessive rate of patients arriving at accident and emergency centres is a major problem facing South African hospitals. Patients are prioritized for medical care through a triage process. Manual systems allow for inconsistency and error. This paper proposes a novel system to automate accident and emergency centre triage and uses this triage score along with an artificial intelligence estimate of patient-doctor time to optimize the queue order. A fuzzy inference system is employed to triage patients and a similar system estimates the time but adapts continuously through fuzzy Q-learning. The optimal queue order is found using a novel procedure based on genetic algorithms. These components are integrated in a simple graphical user interface. Live tests could not be performed but simulations reveal that the average waiting time can be reduced by 48 minutes and priority is given to urgent patients
Deep Dive into Emergency Centre Organization and Automated Triage System.
The excessive rate of patients arriving at accident and emergency centres is a major problem facing South African hospitals. Patients are prioritized for medical care through a triage process. Manual systems allow for inconsistency and error. This paper proposes a novel system to automate accident and emergency centre triage and uses this triage score along with an artificial intelligence estimate of patient-doctor time to optimize the queue order. A fuzzy inference system is employed to triage patients and a similar system estimates the time but adapts continuously through fuzzy Q-learning. The optimal queue order is found using a novel procedure based on genetic algorithms. These components are integrated in a simple graphical user interface. Live tests could not be performed but simulations reveal that the average waiting time can be reduced by 48 minutes and priority is given to urgent patients
South African public hospital Accident and Emergency Centre (AEC) queues are notoriously long. Recent years have seen these hospitals formalizing their medical triage systems, whereby patients are sorted before seeing the doctor to prioritize care to those most urgent. The Cape provinces are beginning to standardize their approaches under the Cape Triage System (CTS) [1]. However, no such standardization exists in the majority of the country. Furthermore, CTS does not make use of technology. The power of modern Computational Intelligence (CI) techniques has aided many industrial and service processes in becoming more automated and uniform [2]. This paper proposes a proof-of-concept system that employs a wide variety of such techniques encompassing machine learning, expert systems and optimization to automate the process of medical triage and digitally aid the management of an AEC in general.
A novel Genetic Algorithm (GA) based approach is applied to the scheduling problem. To find the optimal queue sequence, two factors are considered, namely patient urgency and individual queuing time. Patient urgency is considered based on Triage Scores (TS) as defined by CTS [1]. A Fuzzy Inference System (FIS) is used to automate the calculation of the TS. To estimate how long an individual will wait, it is necessary to have an idea of how long each member ahead of him in the queue will spend with the doctor. This is found using a FIS that is constantly being adapted via reinforcement learning. These technologies are integrated in a user-friendly Graphical User Interface (GUI).
The following section provides a brief background into medical triage, the current systems and how CI techniques have been applied. An overview of the new system is then presented as section 3, before sections 4 through 7 detail its implementation by considering the TS calculations via a FIS, the time predictions via Fuzzy Q-Learning (FQL), the GA based scheduler and the GUI respectively. Sec-tion 8 presents tests and simulations that ratify the system’s success. Section 9 provides a critical discussion of all aspects of the proposal before the paper is concluded.
Public hospitals rarely have the capacity to help patients as they arrive. Triage is the practice of prioritizing patients based on their need for immediate attention and chance of recovery to ensure a maximum number of recuperations [3]. South Africa has no national triage standards. The Western Cape hospitals conform to CTS but their Gauteng counterparts have yet to implement such a framework. Few of the province’s hospitals use any form of triage, which leads to dangerous queue lengths. The Johannesburg General Hospital (JGH) 1 has implemented a triage system based on CTS, explained in section 2.3. The system developed in this paper is based on the JGH but easily generalizes to any hospital.
CI medical triage applications are relatively new. A FIS battle-field triage system employs a similar inference technology to this paper [4]. The Dynasty Triage Advisor is an advanced system that uses Bayesian probability to match symptoms with diseases [5]. An automated triage and hospital check-in system, developed in Canada in 2007, sorts patients through hard coded rules [6]. However systems that use CI inferences to optimize hospital queues appear absent from publically available literature. Similar problems in factories and job-shops have attracted the attention of CI, particularly in the form of stochastic optimization such as GA [7]. Hospital queues do not compare in complexity to these problems and so the application of CI optimization seems to be the natural progression of research in automated triage.
Triage in the AEC of the JGH is performed by nurses. It requires rapid, complex calculations; a task which demands extensive training [8] that heavily burdens hospital resources. The following is a description of their triage process (CTS can be consulted for further detail [1]):
A nurse measures the patient’s vital physiological parameters. The most essential of these are Systolic Blood Pressure (SBP), Heart Rate (HR), Temperature (T°) and Respiration Rate (RR).
Each of these vitals is scored using CTS. Table 1 shows the CTS scores for these vitals.
These scores are then summed and the total defines the triage colour. The nurse may then consider other ailments such as Per Vagina Bleeding (PVB) or localized pain and adjust the colour as necessary.
This information is recorded on paper by the nurse.
The patient then enters the back of the queue unless they are truly urgent.
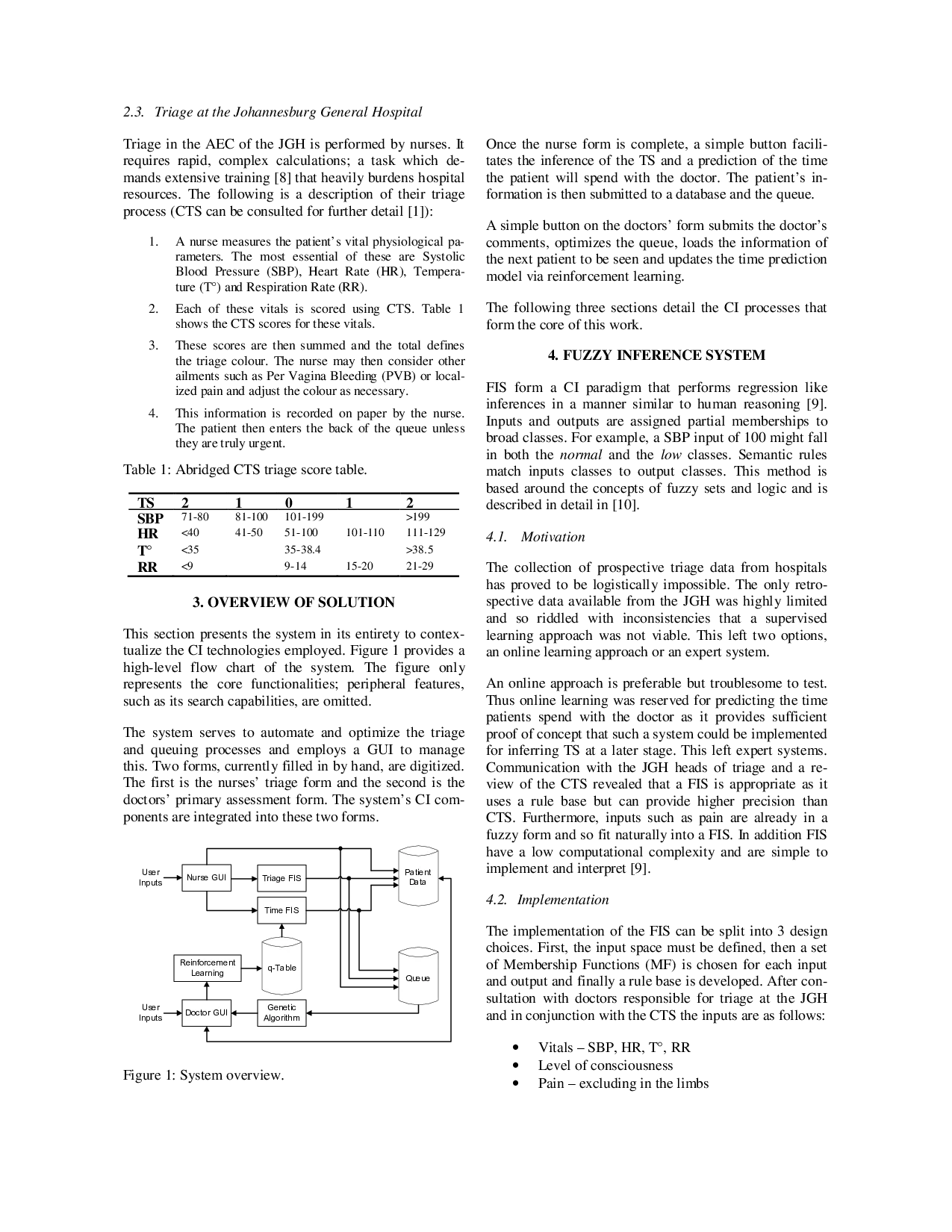
This section presents the system in its entirety to contextualize the CI technologies employed. Figure 1 provides a high-level flow chart of the system. The figure only represents the core functionalities; peripheral features, such as its search capabilities, are omitted.
The system serves to automate and optimize the triage and queuing processes and employs a GUI to manage this. Two forms, curre
…(Full text truncated)…
This content is AI-processed based on ArXiv data.