Emergency Centre Organization and Automated Triage System
The excessive rate of patients arriving at accident and emergency centres is a major problem facing South African hospitals. Patients are prioritized for medical care through a triage process. Manual systems allow for inconsistency and error. This pa…
Authors: ** - 논문에 명시된 저자 정보는 제공되지 않았습니다. (원문에 저자 리스트가 포함되지 않음) **
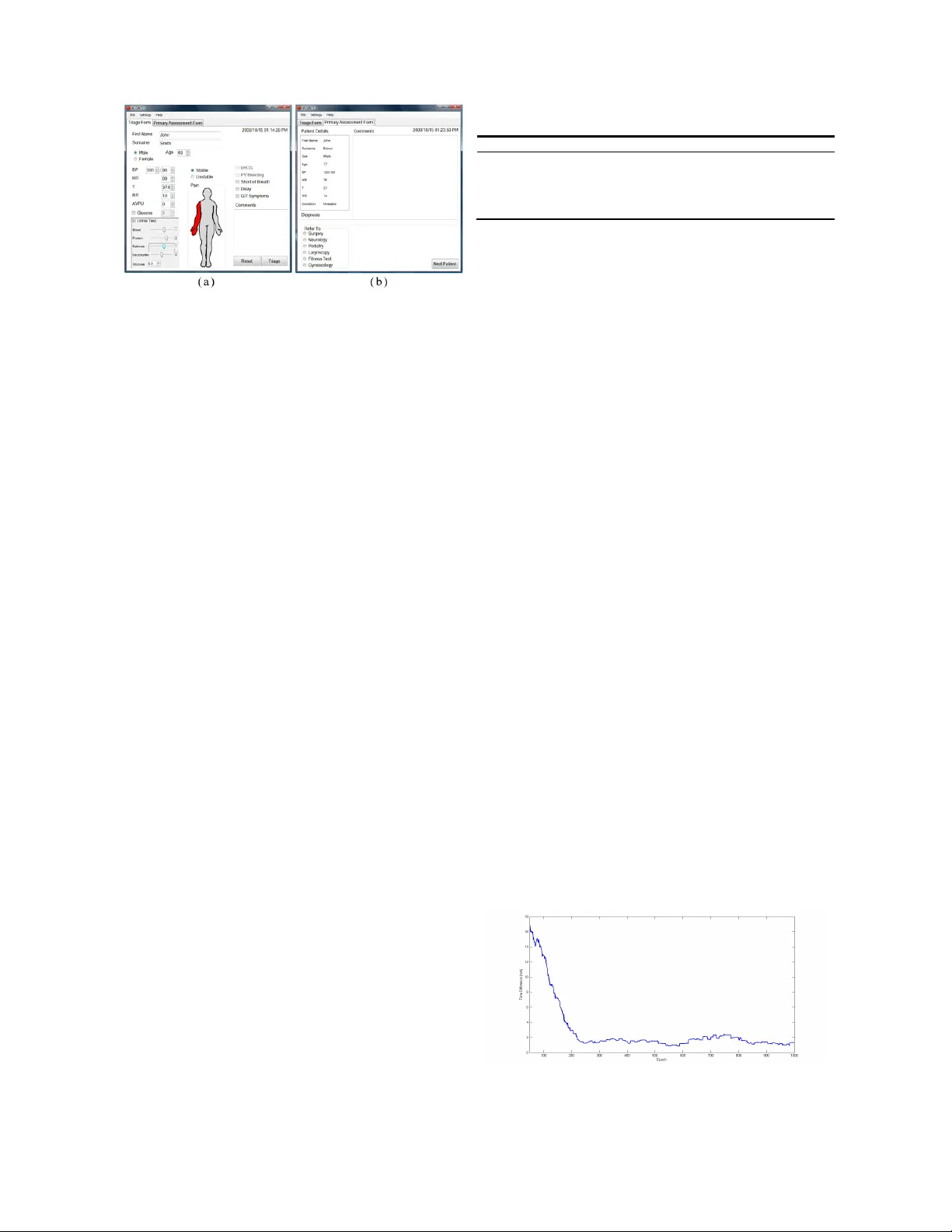
EME RGENCY CENTRE ORGANIZAT I ON AND A UTOM ATED TRIAGE SYSTEM Dan G o ldin g , Lin da W ilson an d T shilid z i Marwala Schoo l o f E l ectr ical & Inf orma tion Eng i neering , Unive rsity o f t he W it w a t ersr and, Priva te Bag 3 , 2050 , J ohann es bu r g , South Afri ca Abstr ac t: The excessi ve ra te of patien ts arriv in g at accident a n d eme rgen cy ce ntres is a maj or probl em facin g South African hospi- tals. Patien ts are prioritiz ed for medic a l c are throu gh a triage proce ss . Man ual s ystems al lo w for in co nsi ste n c y a n d error. This paper propose s a n o vel system to automat e acciden t an d emerge n cy ce n tre t riage an d uses th is t riag e scor e alon g w ith an arti ficial in telli- gen ce est im ate of patien t-doctor tim e to op t im iz e th e queu e or der. A fuzzy in f eren ce system is empl o yed to tr iage pa t ien ts and a simi- lar system estim a tes the time bu t adapts continu ously throu gh f u zzy Q-learn in g. T he optimal qu eue order is foun d usin g a nov el pro- cedure base d on ge n e tic algorithms. T he se compon en t s a re i n te grated in a s im ple gra phical user in terf ace. Live tests coul d n ot be perform ed bu t s im ulati o n s reveal t hat th e av erage wai t in g t im e c an be re du ced by 48 m i nu tes an d priority is given to urgen t pati en ts. Key w ords: Computation al In t elli ge n c e, F uzzy Q-Learn ing, Medic al Triage, Sched ulin g. 1. INTR ODUCTIO N So uth Af ri can pub l ic ho spital Accide nt a n d Em erg enc y Centre (AEC) queue s are n o t o r iously l ong . Re ce nt yea rs have seen these h ospitals form alizing their m edical tr iage sy stems, whereby pati e nts are so rted b e fore seein g the do ct o r to p r ioritize ca re t o th o se most urgent. The Cape prov inces are b eginning to stand a r dize t he i r app roach e s under the Cape T riage S ystem (CT S) [ 1]. Ho w ever, no such stan d ardiza ti on ex ists in the majo rit y of the co untry. Furthe rmo r e , CTS does not make use of t echno l ogy . T h e po w er o f m odern C ompu t a t ion a l I nte l lige n ce (CI ) tech- niques has a i ded many in dustrial and se r v ic e pro c esses i n becom ing more au t om ated a n d unif or m [2]. T his paper prop oses a proof-of-con ce pt system that emp l oys a wide va riet y of such t e ch n iques en c omp assing mac hi ne lea rn - ing, e xpert systems an d op ti miz ation to automa te the proc ess of me d ical triag e and digita ll y ai d t he m anage- me n t of an AEC in ge n era l. A n ov el Ge ne t ic Algorithm (GA) based approach i s ap- plie d to the sch edulin g prob le m . To find the optima l queue sequence, tw o f a ct o rs are c onside red, n am el y pa- tient urge ncy and ind iv idual qu eu i n g ti m e. Pa ti ent u r- ge n cy is considere d base d on Triage Sco r es (TS) as de- f ined by CTS [1]. A Fuzzy Inf ere n ce S ys tem (FIS) is used to automate th e ca l culation of the TS. To estima t e h o w long an in div idu al will w ait, i t is neces sary to have a n idea of h ow lon g each mem ber ahead of him in the queue will spe nd with t he do ctor. T his is f ound using a FIS that is con st antl y being a dapted v i a r einforce m e nt l e ar ning . T h ese techno l ogie s are integ r ated in a user-friend l y G raphical U ser I nterface (G U I ). T h e fo llow i ng section p ro v ides a brief back ground i nto me d ical triag e, t he curren t sy ste ms and how CI technique s have bee n applied. An ov ervie w of the new s y stem is then pre s ented as se ction 3, be fo r e sections 4 through 7 detail its impleme ntati o n b y co n sidering the T S calculation s v i a a FIS, the time predic tions v ia Fuzzy Q-Learning (FQL) , the GA b ase d sche d uler and th e GUI respec t i vely . S ec- tion 8 prese n ts tests and sim ulations that ra ti fy the s ys- tem ’s success. Section 9 prov ides a critical discussio n o f all asp ects of the p r oposal b e fore t he paper i s co ncluded. 2. BACK GR OUN D 2.1. Me di cal triage Pub li c hospita l s rarely have t he cap acity to h elp p atients as they a rr i v e. T ri age is the p r actic e of p rior iti zing pa- tients bas ed o n their need for i mm ediate a ttenti o n a n d cha nc e of re cove r y to ensure a m ax i mum nu mb er of r ecu- pe r ations [3]. South Africa has no national triage stan- dard s. T he Western Cape hospitals co n form to C TS b ut their Gau t eng counte r parts have yet to i mplem ent such a f ramewo r k. F ew o f the prov in ce’s hospitals use any form of triage, whi c h leads t o da n gerou s q ueue l engths. The Jo ha n n esb urg Gen eral Hosp ital (JGH ) 1 ha s i mp l emen t ed a triag e sys t e m base d o n C T S, explained in sec t ion 2.3. The sy stem d e v el oped in this paper is base d o n th e JGH but ea sily ge n eralize s to any hosp it al. 2.2. Curren t solutions CI me dic al triage ap p l icatio n s are r elati v el y n ew. A FI S ba ttle-field t riage system emp l oy s a similar inference techn ology t o thi s p ap er [4]. The D y nast y T ri age A dv is or is an adv an ced system that uses Bayes ian pro bab i lit y t o ma tch s ym ptoms with d isea ses [5]. A n autom ated tr iage and ho s p i tal chec k-in s ystem , deve l ope d in Canada in 2007, sor ts patients th rou gh h ard c oded rules [6]. H ow- eve r sys t e ms that use CI infere n ces to optim i ze h ospita l queue s appe ar abs ent from pu bli ca l ly a va i lab le li terature. Sim ilar prob l ems in facto r ies and jo b-s h op s ha ve attracte d the attentio n of C I , p articularly in th e form of stochastic op t im ization such as G A [7]. Hospital q ue u es do no t comp are i n comp l e xity t o these problems and so the ap- plic ati o n of C I optim iz ation seems t o be t he natural pro- gre s sion of research in au t om ated triage . 1 Now t he Charl ott e Maxeke Joha nnesburg Acad e m i c Hospit a l. 2.3. Triage at the Joha nn esb urg General Hospi t al T ria ge in the AEC of the J GH is pe r formed by nurse s. I t requ i res rap i d, c o mp le x ca l culatio n s; a t ask which de- ma n ds ex t ensi v e training [8] t ha t h eav il y burde ns h osp ital reso ur ce s . T he follo wi ng is a de scriptio n of their tr iage proc ess (CTS can be co nsulted f o r further deta i l [1]): 1. A n urse measu res t he patien t’ s v it al physi o logical pa- rame t ers. The mos t essen tial of these are Sy st oli c Blood Pressu r e ( S B P), Heart Rate (H R ), Tempera- ture (T °) an d Respiratio n Rate ( RR ). 2. Each of the s e vital s is scored usin g CTS. T a ble 1 shows the C TS scores fo r these vitals. 3. Th es e scores are t hen s u mmed a n d the to tal defin es the triage c olou r. The n urse may then consider o ther ailm e n t s s uch as Per Vagin a B leedin g (PVB) or local - ized p ai n a n d ad just the colou r a s n ecessary. 4. Th is infor matio n is recorded on pape r by the nu rse. Th e patien t then e n ter s t he back of the q ueu e unl ess they a r e trul y urgen t . T able 1: Abridg ed CT S triage score tab l e. TS 2 1 0 1 2 SB P 71-8 0 81-1 00 101 -199 >199 HR <40 41-5 0 5 1- 100 101 -110 111- 129 T° <35 35- 38.4 >38. 5 RR <9 9- 14 15-2 0 21- 29 3. O V ERV IEW OF SO L UTIO N T his section prese nt s the s y stem in i ts entirety to con te x- tualize t he CI tec hn ologie s employed . Figure 1 prov ides a high -le ve l fl ow chart of t he s ystem . T he figu r e on l y rep r esen t s t he c o r e functio n aliti es; p eriph er al fea tu res, such as its searc h cap a bilities, are omitte d . T h e system s er ve s to automa te and optim i ze t he triage and queuing pro c esses a n d emp lo ys a GUI t o ma na ge this. T wo form s, currentl y filled in by h a nd, a r e digitize d . T h e first is the nurse s’ tria ge form and the secon d is the do ct o rs’ primary assessment form. The system’s C I com- po nents are integra ted in to these two fo r ms. Nurse GUI User Inputs User Inputs Doctor GUI Triage FIS Time FIS Patient Data q-Table Queue Genetic Algorithm Reinforcement Learning Figu re 1: Sy ste m overview . Once the nurse form is comp lete, a si mp le bu t ton f a cili- tates t he infere nce of the T S and a p rediction of the time the pa t ient wil l sp end with th e doc tor. T he p a t ient’s in - form ation is then subm itt ed to a datab ase and the queue. A simp l e button on the doctors’ f or m su bm its t he doc t or’s comm ents, optim i zes the queu e, loads th e in fo r mation of the nex t pa tient to be s een and updates the time p r e d iction mo del v ia r e i nforceme n t lear ning . T h e fo llowing thre e s e ctions detail th e CI p r oces s es t ha t form t he co r e of this work . 4. FUZZY IN FERENC E SYSTEM FI S form a C I pa r a di gm that perfo r ms regress i on l ike infe rences in a ma n ner si m il ar to h u man re ason i ng [9]. I n pu t s a n d o u t p uts are assig n ed partial m embe r ships to broa d classes. For examp l e, a SBP i nput of 100 m i g ht fall in b oth t he normal and th e low cl a s ses . Semantic rul e s ma tch inp uts classes t o ou t p u t c l asses. T his me thod is base d ar ound t he concepts of fuzzy sets and l og i c and is desc rib ed in detai l in [ 10]. 4.1. Motiv ation T h e c olle cti o n o f pro s pecti v e t riage da ta f r om hospitals has prov e d to be log isticall y i mpo ssi ble . Th e only r etro- spec t ive d a t a a v aila ble from the J GH was hi gh l y lim it ed and so riddled with inc onsistenc ies that a sup erv is ed lear n ing app r oac h was not v i able. T his l ef t tw o optio n s, an on l ine learning a pproa ch or an expert sys tem . An on lin e app roach is preferable but t rou blesome t o test. T hus online lea rnin g was reser v ed for p r e d icting the time pa tients spen d with the doc t or as i t p rov id es suffic ient proo f of con cept that such a system co uld be i mp lemented for in f erring T S at a l ater stage. T h is left exp ert system s. Comm unication wit h t he JGH he ads of triage and a re- v i ew of th e C TS re v e ale d that a FI S is approp ri ate as it uses a rule base b u t c an pro v ide h i ghe r pr ecisio n than CT S. Furthe rmo r e, i nputs such as pa in a re a lre ady in a f uzz y form and so f it naturally int o a FIS . I n addition F IS have a low computatio n al comp l ex i t y an d are si mple t o imp le me nt a n d i n t erp r et [9]. 4.2. Implementatio n T h e i mp lementa tion of the FI S can be split into 3 desig n cho i ces . First, th e input sp ac e must be d efined, then a set of M emb ership Functions (MF) i s chosen fo r e ach in p ut and o utput a nd finally a rul e base is de ve lope d. Af ter con- sultatio n w i th docto rs resp onsible for triage at the JGH and in co njunction with the CT S the inputs ar e as follo ws: • Vitals – SB P, H R, T ° , RR • L evel of con sciousness • Pa i n – ex c l udi ng i n the limb s MF f or th e v itals are b ase d on the C T S ran ges , si mila r t o T able 1. T he cu r v e shape s ar e Ga u ssia n with p l ateau s whos e ce ntres and spreads are adjusted in an ad h o c m an- ner to o ptimize the outp u t. Reg i onal p ains are given a score ba s ed o n l ocatio n and seve ri t y . T he su m o f these score s is us e d as a n inp ut to f uzzy MF dev el o ped in a sim i lar m anner. T h e outpu t MF are b as ed on CTS. T h e rule base is designed arou nd C TS in co nju nction w ith the F I S M F. Additional ru les fo r pa in are based on expe rt op i nions. F u rther rules f ro m C TS are added after th e F I S on an if-t hen b asi s. For examp l e, if t he o u tput is gree n and the pa tient suff ers from PVB, then the outpu t is y ellow. Unlike CT S, the output is not l eft in a fuz z y form. Thus this sy ste m ca n d iffere nti ate seve rit y be tween patients whom C T S classifies as g ree n . T his i ncre ased precision imp r oves the a bil ity of th e sc h e du li ng al go ri thm. 5. FUZZY Q- L E ARN IN G Reinf orcement lear n ing is the unsuperv is ed proce ss whereb y C I agen t s learn to act o ptim al l y in an uncerta i n env i ronm ent [11]. The age n t pe r form s actions by tri al and erro r and i nterpre ts en v ironme n tal reac t ion as reward o r pu nish me nt. Decis ion making paramete rs are t hen altered ac co r dingly . FQL is a spec iali zation of r einforcem ent lear n ing wher e th e de ci sio ns are made b y a FIS and the pa r a me ters altered are the weig hts of t he rule ba se. 5.1. FQL algorithm FQL i s a c omp l ex m athema t ical procedure a n d its details ca n b e found in [ 11 ]. T h is sec t ion prov ides a sh o r t high lev el e xpla nation of w ha t FQL is concep t uall y . FQL revo l ves around the q-table , a tab le of weights repre- senting all p o ssi b l e rules connecting th e input sp a ce t o the ou t p u t space . I ts r ows are th e antece d ents a nd colu m ns the con s equen t s. I n fuzzy logic, a n i np ut vector can acti- va te many antecede nt s [9]. FQL chooses the best con se - quent fo r a gi v en set of antece d en t s. Th i s is done b y an Exp l oratio n -Exp loitation Function (EE F). Exp loration me ans ch o osi ng a c on sequ en t at random , exploitation me ans choos in g the conse quent with the highes t value on the q - table. T he E EF de f ines the probab i lit y of the co nse - quent being ch o sen by either exploratio n or exploita ti o n. An ac t ion is then performe d using this c o nsequent and the env i ronm ent resp on ds wit h a re wa rd which is used t o up date the we ight of th e cho s e n c onsequent. 5.2. Motivation No data are availab le on which t o build a n e xpert syste m or train a mo de l by su perv i sed learning. Howev er it does seem plausib le th at the time spent w ith a d octor is s ome- what influence d by measureab l e fa ct ors . Th e po w er of FQL i s that if th ere are rules gove rni ng t he behav i our of this sy s t e m , t hey will be f ound. T h e on l ine l ea r ning c a pa cit y means that no n -s t ationar y proc esses, which this m i g ht we l l be , ca n be m od elled. Furthe rmo r e , d i ffe rent s ystem s can be trained to m ode l diffe rent do ctors. 5.3. Implementatio n T o asce rtain what inputs sh ould be considered, and i f th e mo del should be in fe r enc e based or stocha sti c, would requ i re live t esting in a hospita l e n vironm ent. This was a log isti ca l impos sibility for this study and so i np uts were arb itraril y selec t ed to be the pa t ient severity and the p a- tient ag e. This selecti o n i s inco nsequential as adding in- pu t s is tri v ial . T h e EEF, tweake d by the tests in sec- tion 8.2, is des cri b ed by (1) ≥ < − = 250 w hen 05 . 0 250 when 003 8 . 0 1 t t t ε (1) Whe re: ε = probab i lit y of exp l ora t ion t = ep o ch No te that the p robabilit y of ex p l o i tation is thus 1 - ε . Henc e t he policy is t o begin with a high pro b ab ili t y of exp l o ration, allow ing the sy st e m to find g lobal op ti ma , and linearly decr ease this to a 5 % cha nce by ep oc h 250. 6. SCH EDULIN G ALGOR ITHM Sc hedulin g is the pr i orit izing , t im i ng, and s eq u encing of wo r k [12]. Said another way, sc h eduling is the p r ocess of f inding an optimal seque n ce. Man y algo rith m s are a va il - ab le, fr om d e t erministic to stoc hastic, si ng le line to mu l ti- line, s imple priorit y b ase d to comp l ex orders fo r j ob- shop s. Prudent u se of sched u li ng can drastically reduce waiting time s, save mo ne y and increa s e op erational effi- ciency . It ap plies e q ually to ma nu f acture a s to ser v ic e industrie s, t he l at ter being o ur concern. Example s r ange f rom algo rith m s gove rn ing call centres t o the ord er ing of instructio ns in d igital pro cessing [13]. Clea r y AEC queue s can draw from th e b ene f its o f sche d uling . 6.1. Constraints and consider a tions I n a h ospital queue, t he wo rk to be sequenc ed is t he wait- ing patie nts. Eac h m ember h as t wo factor s t hat nee d t o be co nsidered: urge nc y and waiting t im e. T ogether the s e f actors determine pati ent pr i orit y and th us c an be use d t o def in e the optim al sequence. Both are ess ential. I rre ve rsi - ble da mag e can occu r if urgent patients are m ade to wait too l ong. Howev e r, pa t ients that are le ss urgent can n ot be expe cted to w ait fo re v er and thus t he t ime spen t i n t he queue m ust be co nsidered. Unlike j ob- sh ops where ce r tain jobs have t o be d one be- fore othe rs are p ossible , hospita l queue s can b e arra n ged in a ny per m utati o n. This me ans that f o r a queue of 20 pa tients, a reason a ble numb er for the JGH , the search spac e comp ri ses a pp roximatel y 2. 5 x 10 18 sequence s. T his make s the use of stochastic app r oac h es n e cessa ry. GA was i nitially chosen for its ab il ity t o de al with seque ncing native l y [14]. Ho w ev er, the use of a nov el al go rith m that maps seque n ces to nu mb ers me ans any st oc h astic o p t im i - za tion c an b e used. G A is ch ose n f or its simp licit y and widely availab le program mi ng to o l boxes. G A i s a st oc hastic op t i m isati on t ec h nique b ased on bio- log ic al evolutio n . The co nc ept of survival of t he fittest is used by mo d elling a pop ulati on ’s fitnes s a f ter the fun ct ion to b e optim i zed, which is he nce known as the f it ness f unc tion. Th e indi v idual memb ers of the p opu l ation (each of which is a potential solution) undergo the bi o l og ical proc esses of s elec t ion, rec ombinatio n an d m u tatio n t o form n ew genera t ions which converge on gl oba l op ti ma . Refe rence [15] prov ide s a deta il ed ex planati o n of GA. 6.2. Nove l Algorithm F i tness f unction: A nov e l fitness fu ncti o n is used that ac co u nts f o r p at ient u rge n cy as well as wa iti ng t imes and is desc ri b ed b y (2). ∑ ∑ = − = + − + n i i k ek ai i t t t T 1 1 1 ) )( 1 ( (2) Whe re: n = n um ber of patients in queu e T i = T S of p atient i t = current ti m e t ai = tim e that pa tient i arri v e d t ek = tim e that p atient k i s ex p ec t ed t o s pend with the d oc tor T his e q uation assigns a va lu e t o a queue orde r by mu l ti- ply ing each patient’s ur ge n c y wi th the tota l t im e the y spen d waiting. T i +1 i s the T S , i.e. p at ien t urge ncy . The additional o ne ensure s that t he ti m e in forma tion is no t los t in t he case where the T S is z ero. T h e total time is broke n up into th e t im e the pa ti ent has alread y w aited, t – t ai , and the ti m e the patient will still wa i t i.e. t he sum of the time eve r y pe rson ahead in t he queue is expec t ed to spend with the do ctor. Thus t he goal of the GA is to find the se- quenc e for which (2) y i elds t he lowest res u lt . One draw- back of th e G A is sp eed. Th e algo ri th m takes aro und 30 s T able 2: T he first 8 (o f 24) perm utations as see n by the mapp i ng algor it hm gi ve n n = 4. Index Sequence 1 1 2 3 4 2 1 2 4 3 3 1 3 2 4 4 1 3 4 2 5 1 4 2 3 6 1 4 3 2 7 2 1 3 4 8 2 1 4 3 Figu re 2: Pseu do-cod e of the m apping algorithm . for an excep ti ona l l y long q ueu e of 10 0 membe r s. Whilst this is s low, it is perf ec tly r easonab l e when conside r ing the app l icatio n , a f ter all it will take a p ati ent longe r than 30 s to leav e th e doc t ors room . Map p ing function: G A g enerates a pop u latio n o f nu m- be rs, not sequ en ces. Th us a f un ction is required to m a p these numbe rs to all possible per m utations of a gi ve n queue leng th. Th e functio n arra n ge s p er mutations so as to m i nim iz e ch a nge betw e en perm utations of co n secutive indices. T his arrang e me nt leads to a smoother fun ct ion which is ea si er to optim i ze [16]. T able 2 shows a samp l e of p ermutati o ns and there co rr e s ponding indices. T h e GA gen er a t es indices but the fitness function require s sequ ences. An alg orit hm t hat finds a sequence gi ve n an index and the num ber of elements ha s been dev el op ed and is describ ed by Figure 2. I t is ba s ed on the fact that num - be rs are grou ped in batc he s of p ! where p is n minus the elem ent numb er. F or e xample , notice the g roup of si x on es in the first c olumn of t he sequence s in T a ble 2. T his is elem ent o n e where n = 4 t hus p! = 6. He nce the q uo- tient of di v idin g the inde x by p ! is one less than the num- be r f or that element. T he foll o win g e l ements ar e found throug h the same p r ocess, but instea d of t he i ndex the rem ainder is di v id e d. T h e only excep tion oc curs when there is no remainder. I n th is ca s e it is not n ece s sar y t o add 1 and p ! is considere d the rem ainder instead o f zero . 7. IN T ERFACE AND IMPLEME NTATIO N 7.1. Int erfac e Whilst no t co re to the s o l ution, the GUI demonstrates ho w the se co mp le x and po we r fu l CI tools ca n be inte - gra ted i nto a si mp l e i nterface . T he GUI has two m ain form s, sho w n in Figure 3 . The forms are desig n ed to be as user-f riendly as possible. It is esse nt ial t ha t the use o f an elec tronic fo rm does no t hinder the n urse in any way . T hus th e form is desig ne d t o be quick and simple to use, and elim inates the need fo r fr ee t yping wherev e r po ssi b l e. Inputs: index ( x ) s eque nce size ( n ) Output: s eque nce Begin: creat e pool of numbers 1 t o n i = 0 R epe at n times incre m e nt i ref i s quo t ient of x /( n – i ) ! rem i s re m ai nder of x /( n – i )! if rem = 0 then r em is set to ( n – i )! else i ncrement ref digit i of output is digit ref of pool remove di git ref from pool s et x to be rem end End . Figu re 3: Screen shots o f the G U I. T he nur se fo r m is sho wn in (a) and (b) sho ws the docto r form. T h e p ain interf ace sim ply r equires the nurse to click on the anatom ic al regio n wh er e t he patient fee ls pain. T his turns y ellow to in dicate mild pa in, and another click t urns it red f or severe p ain. T h e doctor’s form automatically provide s information such as patient nam e a nd v itals. T he do ctors’ no t es ar e no w t yp ed elim i nating th eir noto rious problem of ill e gi b l e hand- writing. T h e Next P atient button l oa ds this info r ma- tion and triggers the necessary CI , which tells th e docto r who is next fr o m t he re-op t i m ized queue . 7.2. Deve lopment T hr ee languages have b een used in th e s y st em’s deve l - opm ent. T he GUI is programm ed in C# . Th i s lang uage is desig ned for dev elopers to be ab l e to produce applica t ions in m inim al time. Being o b j ect oriente d , it al l ows for high l y mo dular pr ogramm ing fa cilit ating fu t ure expan- sio n. T he in form at ion is stored using MsSQL . SQL i s a tried and te st ed datab asin g lang u a g e w hich can b e ac- ce ssed na t i vely in C# . I t is used for reliabili ty and ea se of deve lop me n t. Finally , the te chnical CI com p onents , t he co r e of th e sy st em, ar e develope d in Matlab as it g r ace- f ull y handles comp l ex num er ical ca l culations. Further- mo r e, Matlab ha s too l bo x es that cate r fo r FIS and GA and has a powerfu l v isualizatio n functio n alit y whi ch i s a tre- me n do us aid whe n t esting v ia abstract simu l ations. 8. TESTS AN D SIM UL ATI ONS T i me and logistics do no t allo w fo r a thoroug h , l iv e test- ing of the system . For this reaso n a s e r ie s of sim ulations are used to test e ac h C I aspe ct ind iv iduall y . 8.1. Triage scor e infere nce Sim ulations are b ased on data collec ted f rom the J GH . Comp aring results of the FIS w ith those from t he J GH is f util e due t o the inco nsistencies o f th e nu rse s, so they are comp ared w ith C T S instead. Pain is co n sidered separ atel y as CT S isn’t spec i fic abo ut i t. Succe ss is m easure d against comm on metrics for under- tria g e (less t han 5 % o f ca ses) and over- tri a g e (l ess t han 50 % of cases) [ 17]. Table 3 sho ws the results of t hese tests. T able 3: Perce ntage of under a n d ove r tr iage . Unde r Tri age Co rr ect T riage Over T ri age No Pain 2 96 2 Low Pai n 1 91 8 Medi um P ain 0 60 40 H ig h Pain 0 37 63 8.2. Predic tio n of time to be s pent w ith doctor Neithe r lite rature nor d at a is av ail ab l e o n these predic- tions. This test is pure l y a proo f -of-co n cept. Howev er, it is possible t ha t no r elations hip d eterm in es h ow lon g doc- tors spen d wi th pa ti ents, o r that the relation ship is sto- cha st ic in whi ch ca se st atistica l m odelling m ight be pref- erable . I t is not pos si ble to k n ow this witho ut running tests in a live hosp i tal e n vir onment. I t is assumed that th ere is at lea st some rela ti onship gov- erning th is ti m e and t ha t it ca n be in f erre d fr om symp t o - ma tic and dem o graphic info r mation . To test the o nline lear n ing capabilities, r andom FIS m odels a r e ma de and data are produ ced u sing these mo d els. The s ystem is then trained and the simila ri ty betwe en th e tr aining sy s tem and the online l e arning sy stem is inve st igated. I n all ca se s, the FQL model as sig ns i ts highest v alues on the q-ta ble t o the rules of the FIS it is learning f ro m . Te sts revea l that an EE F which reduce s e xp l o r ation t o a prob- ab ilit y of 5 % after 200 epoc h s pro duces t he best resu l ts. Figu re 4 sh o w s a slidi ng aver a ge ( ove r 100 epochs) of the time d iff er e nc es be t ween the simula ti on a n d the FQ L mo del as it learn s. Once the mo del ha s settled, the av er- age absolute d iff ere n ce is less than 4 m in. 8.3. Scheduling T h e data c ollec ted form t he J GH pro v ides t he t im es that pa tients arr ive a nd the ti me that t hey see the d octor. Un- fortunate l y th e t i m e s pent with the docto r is not re co rded. I t i s as su med that the co nsecuti v e tim es betwe en whe n pa tients see the d oc t or in dicate the ti me s pe n t w i th t he do ct o r. To si m ul ate t he ou t put of th e online learning proc ess, noise is a dd ed to these ti m e s as characte rized b y the tests in sectio n 8.2. Figure 5 show s the waiting tim es of a qu eue of 17 pa t ients w it h a n d w ithout sche d uling. T h e average wa it ing t im e from t he J GH data is 169 m in . Sc hedulin g re d uc es this t o 12 1 min. Figu re 4: Tim e difference o f a F IS training a FQL m od el. Figu re 5: Wai ting time witho u t s che duli ng (solid blue line) and with sche d uling (dash ed black line). 9. C RITIC AL ANALY SIS 9.1. Evaluation T h e pro po sed solution ha s achieve d the goal of b eing a proo f- of-co nce pt automate d t riag e system . Th e C I te ch- no l ogie s at the core of t he system h ave b e en teste d and sho w pro m isi ng results. Simula tions reveal that queu e op t im ization can reduce th e average patient waiting ti me by 48 m i nutes. The FQ L s ystem h as prov ed to be able t o lear n f r om a rule based en v ironment to predict the tim e a pa tient will s p end wit h the doc tor o n a ve r age to withi n 4 m inut es of th e tru e ti me . The t riage sys t e m has r e du ced under- t riage to l ess than 2 %. Over-triag e is more difficult to interp r et as i nc r ea s ed pa in should increa s e t he T S. Onl y in c ase s of severe pa in does th e FIS tri age higher th an CT S fo r more than 50 % o f c ases; howeve r C TS is like l y to unde r -tria ge in these c ases which is why i t recomm ends nurse s p ri o ritize p atie nt w ith p ain highe r than th eir T S. T h e system serves as sufficient proof that such a pro duct is worth t esting in a live h osp i tal env iron m ent. 9.2. F uture W o rk T h ere i s the po tential t o i mpleme n t nume r o u s useful fea- tures from aut omatic calib rati o n of nu rsing equipm ent t o enha ncing the automa t ed triage sy ste m with natural l an - gu a ge processing . Th e mo s t pressing w ork howe ve r is t he running of live tests. Th e s ystem ne eds minor a l teratio n s, ma in l y t o do with n etw ork in g, t o be ready for te sting i n a ho s pital e n v ir o n m ent. Only with s uch tests can t he C I comp onents truly be e va lu ated and improv ed. Furt he r wo r k into the r einforcem ent le arning a spects is al so rec- omm ended but ca n not be d o n e with o ut l iv e tests. T ests will show what inputs are approp ri ate for t he tim e predic- tor. FQL sh ould also b e i m pleme nted i n th e tri ag e predic- tion sta ge. Bo th FQL mo d els sho uld allow for the MF shap es to be tra i ned in ad dition to the rule ba se. 10. CO N CLU SION CI too ls can hav e a po w erful impact on t he runnin g of AEC. I nference mo dels r emov e nurse bia s and human erro r from t he t riage pr oc ess and scheduling reduces pa- tient wait i ng ti m e and increa s es efficien c y of t he h ospital env i ronm ent. Th e deve l o pe d system sh ows p rom i sing results th rou gh si mula tions. Analysis of these results sho ws that t his is a p r o du ct well wo rt h test in g in a hos pi - tal env ir o n ment to truly ascertain what impact suc h a s ys- tem ca n ha ve on the m edic al indust ry . ACK NOWLEDGEMEN T T h e author a ck n ow ledges Prof . Boffar d and Dr. M otarra of the JGH for the ir help and adv i ce reg arding c u rrent triag e s ys te ms in South Af ri ca and accomm od ating the co llection of triage data. REFERENC ES [1] S. B. G o ttschalk, D. Woo d, S. D e Vries , L. A. Wa ll is , “The c ap e triage score: a n ew triage sy stem”, Eme r- gency Medicine Journa l , Vol. 2 3, pg . 1 49–1 5 3, 2006. [2] A. Kus iak, C o m putati onal inte lligence i n de si gn and manufac t ur i ng , Wi l ey -IE EE, 20 00 . [3] J. C . Bri l lman, D. Doez e ma, D . Tan e nbu r g, “ Limita- ti ons in predic t ing need fo r e m ergent ca r e and hosp it al admission” , Ann als of emerge nc y m ed i cine , V ol. 27, I s- sue 4 , p g. 493-500, 1996. [4] S. M. W en de l ken , S . P . McG rath,“A m e dica l asse ss- ment alg or it hm fo r aut o m a t ed remote triage” , 2 5 th IEEE EMBS , Vol. 4, pg . 3630–36 33, 2003. [5] A, Biss, Dynas t y triage advisor enab l es med i ca l d eci- sio n - suppo rt , 20 02. http: // dssreso ur ces . co m/ ca- ses/dy nas t y . htm l, l ast a cc e ssed 14 / 08/08. [6] H. Ali, E . Quach , P. Sabat i ni, Automa t ed triage check- i n , EE4BI 5 Biomedica l De sign P ro j ec t, 20 07 . [7] C. Bier with, D. C. Mat t fe l d, “Pro d uction sche d ul i ng and r e s ch eduling wi th g enetic algo r ithms” , E volu t io na ry Co mpu ting , Vol . 7, No. 1, pg. 1 –17, 2 007. [8] J. Cioffi, “Triag e dec i si o n mak i ng: educat i ona l st rate- gies” , Acciden t and Emerge ncy Nur sing , Vol . 7, I s sue 2, pg. 106–111 , 1999. [9] G. Cas tellano, A . M. Fanell i , C. Mencar, Design o f tra n sparent fuzzy mamdan i systems in Design and ap- plication of hybr i d inte l ligen t s y s tems , I OS Print, Am- sterdam, pg . 468–476, 2003. [10] L . A . Zadeh, “ Fu zzy Se ts”, In f orma ti on and con t rol , Vol. 8, pg . 338–353 , 1965 . [11] A . Bona ri ni, A . L azar i c , F. Montrone , M. Rest elli , “Re- i nforcem ent distribu t ion i n fuzzy Q -learn in g” , Fu zz y sets and s y stems , 2008 . To Ap p ea r. [12] M . Dav i s, J . Hei n ek e, Operati o ns manage ment, inte- grating m anufacturing and s er vi ces , McG raw-Hi l l I r - win, New Y ork, 5 th editio n, 2 00 5. [13] M . Pinedo , P l ann ing an d s c hedu li ng i n manuf act u r e and serv i ce s , Sp ringer, 2005 . [14] S. N. S i v anandam, M. Kannan, “Job sequen ce mo delli ng using g e netic algo rit hms” , A cadem ic open i nterne t j ou rn al , Vol. 12, 2004 . [15] T. M un a kata, F un damen t als of new artif i ci al intelli- gence – neural, ev ol u t ion ar y, f uzzy and more , S pr i nger- Verlang , Lo ndon, 2008 . [16] S. Th r un, L . K . Sau l, Adva nce s i n neuro i nf o rma ti on proc es sing system s , MIT pre ss, 2004 . [17] G. F. S. L i ng , A. Urias, “Medica l tri a ge a ssistan t, a di- agno stic sensor suite f or f ar fo r ward hosp i tals”, RTO - MP-HFM - 109 S t. Pe t e Beach – USA , 2004 .
Original Paper
Loading high-quality paper...
Comments & Academic Discussion
Loading comments...
Leave a Comment