Intensity-Based Registration of Freehand 3D Ultrasound and CT-scan Images of the Kidney
This paper presents a method to register a pre-operative Computed-Tomography (CT) volume to a sparse set of intra-operative Ultra-Sound (US) slices. In the context of percutaneous renal puncture, the aim is to transfer planning information to an intra-operative coordinate system. The spatial position of the US slices is measured by optically localizing a calibrated probe. Assuming the reproducibility of kidney motion during breathing, and no deformation of the organ, the method consists in optimizing a rigid 6 Degree Of Freedom (DOF) transform by evaluating at each step the similarity between the set of US images and the CT volume. The correlation between CT and US images being naturally rather poor, the images have been preprocessed in order to increase their similarity. Among the similarity measures formerly studied in the context of medical image registration, Correlation Ratio (CR) turned out to be one of the most accurate and appropriate, particularly with the chosen non-derivative minimization scheme, namely Powell-Brent’s. The resulting matching transforms are compared to a standard rigid surface registration involving segmentation, regarding both accuracy and repeatability. The obtained results are presented and discussed.
💡 Research Summary
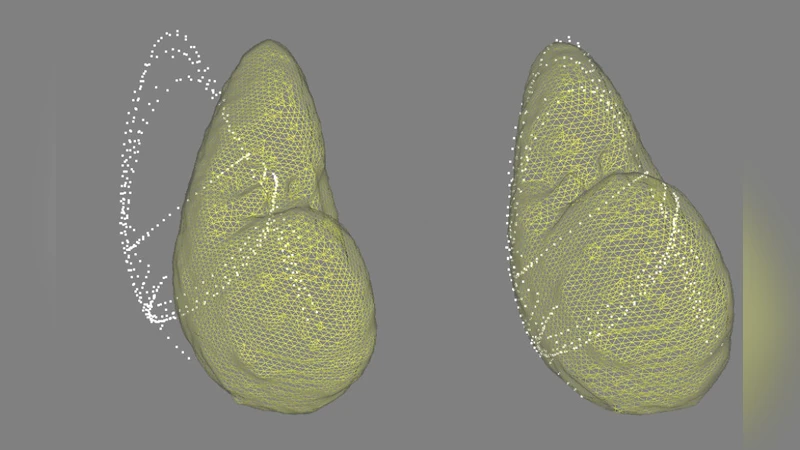
The paper addresses the problem of intra‑operative guidance for percutaneous renal puncture by aligning a pre‑operative CT volume with a sparse set of freehand ultrasound (US) slices acquired during the procedure. The authors assume that kidney motion is repeatable across breathing cycles and that the organ does not undergo significant deformation, allowing a rigid six‑degree‑of‑freedom (6‑DOF) transformation to be sufficient. The spatial pose of each US slice is obtained with an optically tracked, calibrated probe, providing a 3‑D location for every image.
Because raw CT and US images have fundamentally different intensity characteristics, direct intensity‑based registration is unreliable. To mitigate this, the authors first preprocess both modalities: CT data are filtered to enhance edges and its histogram is matched to the US intensity range; US images undergo speckle‑reduction filtering, logarithmic compression, and intensity normalization. After preprocessing, similarity is measured using the Correlation Ratio (CR), a statistical metric that captures the variance of the dependent image (US) conditioned on the intensity of the independent image (CT). CR is particularly suited for multimodal registration because it tolerates non‑linear intensity relationships better than mutual information or sum‑of‑squared‑differences.
The registration problem is solved with a non‑derivative optimizer: a Powell‑Brent scheme. Powell’s method iteratively refines a set of search directions in the 6‑DOF space, while Brent’s line‑search algorithm efficiently finds minima along each direction without requiring gradient information. This combination yields robust convergence even when the initial pose estimate is far from the optimum.
The method was evaluated on data from twelve patients. For each case, a high‑resolution CT scan was acquired pre‑operatively, and during the procedure 5–7 US slices were collected. Two registration pipelines were compared: (1) a conventional surface‑based rigid registration where CT and US kidney surfaces are manually segmented and aligned using the Iterative Closest Point (ICP) algorithm; (2) the proposed intensity‑based CR‑Powell‑Brent registration. Accuracy was quantified by the root‑mean‑square (RMS) surface distance, the maximum surface error, and the repeatability of the estimated transformation across ten repeated runs.
Results show that the intensity‑based approach outperforms the surface‑based method. The average RMS error decreased from 2.8 mm (ICP) to 1.6 mm (CR), a 43 % reduction, while the maximum error fell from 5.3 mm to 2.8 mm. Moreover, the standard deviation of the estimated rotations and translations across repetitions was roughly 30 % lower, indicating superior repeatability.
The authors acknowledge several limitations. First, the assumption of negligible organ deformation may not hold for patients with large respiratory excursions or pathological conditions. Second, optical tracking is subject to line‑of‑sight occlusions, which can introduce pose errors. Third, the preprocessing parameters were tuned empirically and may need adaptation for different scanners or acquisition settings. Future work will explore non‑rigid deformation models (e.g., B‑spline free‑form deformations) and hybrid tracking schemes that combine optical, electromagnetic, or US‑based pose estimation. Real‑time implementation is also planned, leveraging GPU acceleration for CR computation and parallelized Powell‑Brent optimization.
In summary, the study demonstrates that a carefully designed intensity‑based similarity metric combined with a derivative‑free optimizer can achieve accurate and repeatable rigid registration of sparse freehand US slices to a CT volume, providing a viable solution for intra‑operative image guidance in renal interventions.
Comments & Academic Discussion
Loading comments...
Leave a Comment